










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkIntroduction
Results from global studies show that the majority of children do not meet the recommended health-related level of physical activity (PA) (Chin, & Edginton, 2014; WHO, 2012). Nelson, Neumark-Stzainer, Hannan, Sirard, & Story (2006) reported substantial longitudinal changes in moderate to vigorous PA, particularly among girls (decreasing 5.9-4.9 hours/week from early to mid-adolescence and 5.1-3.5 hours/week from mid- to late adolescence). Disturbingly notable is the reported decline in PA among preschool and primary school children (McKenzie et al., 1997). In this category, the majority of children do not meet the recommended health-related PA level recommended by World health Organization (Duncan, Al-Nakeeb, Woodfield, & Lyons, 2007). This decline in PA engagement is especially relevant in contemporary life, which promotes sedentary behaviour. In turn, sedentary behaviour has a negative effect on children’s physical health, body mass index (BMI), muscle strength and tone, spine and joint flexibility, and proper bone density (Biddle, & Asare, 2011; Castro-Sánchez et al., 2017), putting them at risk of serious chronic diseases in later life, including ischemic heart disease and type II diabetes (USDHHS, 2010). In addition, an individual’s mental state and self-perception have been shown to be associated to PA levels in school-age children, including anxiety and depression, physical (sport) competence, and identity (Strong et al., 2005). Furthermore, the literature continues to support the enhancement of children’s cognitive performance resulting from participation in PA (Davis et al., 2011; Sibley, & Etnier, 2003).
Extant research has found that the place where PA levels of school children can be most effectively impacted is the school, during the physical education lesson (Kahn et al., 2002; Kruk, 2007; Marshall, & Hardman, 2006). However, some researchers argue that low PA levels are consequence of the curricular content taught during the PE class, which has a major focus on motor skill development (Smith, Nichols, Biggerstaff, & DiMarco, 2009). Furthermore, the level of PA is proportionally higher when children are given the opportunity to play active games and experience fun (Arnett, & Lutz, 2003; Hastie, & Trost, 2002; McKenzie et al., 2006; West, & Shores, 2008; Wickel, & Eisenmann, 2007). Particularly important to younger, primary school children is the opportunity to engage in physical activities that they perceive as meaningful and enjoyable, where they can fully reveal their abilities in a physically active motivating environment (Bailey et al., 2009; Løndal, 2011). Promoting PA in schools poses a challenge for PE teachers who have to balance engaging students in adequate amounts of PA during PE lessons, and educating them about the knowledge and skills needed to maintain physical activity throughout life as required by the PE curriculum (Fairclough, & Stratton, 2005). Including a daily structured in-class PA break (in addition to the students’ regularly scheduled PE lessons) may be a good solution to increase the level of PA in young children.
Several studies have confirmed that recess can be a valuable opportunity for primary school children to increase PA levels (Roberts, Fairclough, Ridgers, & Porteous, 2012). However, the activities that students participate in during recess or other outside-of-class-breaks (e.g., before school, lunch period, etc.) do not provide a high activity time in many primary schools (Cardon et al., 2012; Lee, Burgeson, Fulton, & Spain, 2006). Creating safe and friendly play environments is essential as evidenced by research, which shows that primary school children are more physically active in large area playgrounds than in small ones (Escalante, Backx, Saavedra, García-Hermoso, & Domínguez, 2012). Jennings-Aburto et al. (2009) identified the following barriers that negatively impact engaging in PA during these breaks in the school day: (a) time dedicated to purchasing and consuming food; (b) the absence of sports equipment; (c) a no running or playing policy due to overcrowding; (d) lack of organization or teacher participation in children’s PA (Jennings-Aburto et al. 2009). In a review of studies (n = 12) in which PA during school breaks was examined, Stanley, Ridley, & Dolman (2012) found some relationships among level of PA, gender, age, and access to play space and PA programs; these researchers, however, suggest that much still remains unexplored about class breaks in schools and PA opportunities.
Considerable steps have already been made to increase PA levels during school recess periods. Studies show that providing game equipment is an effective means of increasing children’s PA levels (Verstraete, Cardon, De Clercq, & De Bourdeaudhuij, 2006). Simple and effective low-cost solutions for promoting PA during breaks can be achieved by providing multicolour playground markings for games, including netball, football, and short tennis (Stratton, & Mullan, 2005).
Some other strategies involving digital facilities are leading the way in promoting interactive PA. Brain Breaks, an interactive online resource, are 5-9 minute web-based structured classroom PA breaks that have been developed to help revitalize student behavior through moving and engage students cognitively in the content area of health, specifically designed to be used in the classroom setting. Brain Breaks include national, dance and sport movements. Students not only have the opportunity to be physically active during Brain Breaks, but also master new motor skills while reinforcing and strengthening multidisciplinary curricular and non-curricular learning by integrating PE and health lessons with classroom learning (Chin, Edginton, & Tang, 2013). With Brain Breaks, accessible through online streaming, teachers have an instant resource available, requiring no additional preparation time. Computers, desktops, laptops, tablets, white boards and smart phones are all examples of internet-enabled devices that can access Brain Breaks in the classroom. Digital content instruction is in English, which does not pose a barrier and re-confirms movement as the universal language.
Classroom Brain Breaks are not interchangeable with recess. Rather, they are structured PA breaks designed for the classroom (HOPSports, 2017). Recess is best situated for unstructured play (Keeler, 2015), which is an extremely valuable and essential component to a child’s development (Lillard et al., 2013). In contrast, structured PA classroom breaks are designed to promote optimal learning by becoming an integral part of the classroom environment (Goh, Hannon, Webster, & Podlog, 2017).
Unique to the Brain Breaks used in this study is the emphasis on developing the whole child through a multi-layered approach. Increasingly, classroom teachers are tasked with providing health education as well as PE, character development and safety awareness as part of their curriculum and classroom environment. Brain Breaks provide an interactive experience for students and a connective platform for teachers. PA breaks are perceived as an integral part of the learning experience rather than an interruption (Goh et al., 2017). Certainly, as intuitively expected, classroom management, student health and behaviour, test scores, engagement and energy levels all receive a boost from inserting PA routinely throughout the school day. What is noteworthy about Brain Breaks are the tangible aspects of PA cognitively (advancing language, art, music and culture), as well as the intangible and underlying aspects of PA to promote self-motivation and confidence.
To date, an insufficient body of research exists substantiating the effect of classroom Brain Breaks to promote children’s knowledge acquisition and motivational application of PA and healthy habits as cornerstones of lifelong health and well-being. Hence, this study is intended to pertain to this framework, and it will use available research on video games to inform the hypothesis and expected outcomes. While technology renders the younger generation stationary and health compromised, it also holds the key to relevant and exciting physical activities and health education. Active videogames (AVGs) and digital Brain Breaks, which combine screen time with PA, can help to reduce physical inactivity.
Interactive Brain Breaks are administered where children spend most of their time - in the classroom. As such, it seems like the ideal place and time to teach healthy habits. Children will readily engage and continue to participate in physical activities and health lessons that are varied, fun, interchangeable and incorporate music choice. The challenge and opportunity is to find ways to develop technology which promotes and encourages repeated participation in PA. Brain Breaks have demonstrated the ability to positively influence self-attitude, knowledge acquisition and application, and contribute to sustainable behavioural change (West, & Shores, 2014). Along with the Brain Breaks, the instrument measuring its outcomes, the Attitude toward Physical Activity Scale (APAS), was created and validated by Mok et al. (2015).
The APAS was based on Welk’s (1999) youth physical activity promotion model (YPAPA). The instrument measures attitudes and perceptions regarding different aspects on engagement in physical activity: children’s perceptions of, attitudes towards, motivation for physical activity and self-confidence and specific academic knowledge acquired. The emphasis is made on physical activity using video games.
The aim of the current study was to investigate the effects of providing Brain Breaks® video exercise lessons to primary school children during class breaks. The study explored the effect that such lessons had on the students’ attitudes toward physical activity, physical self-efficacy, and health-related academic knowledge acquired.
Methods
Participants
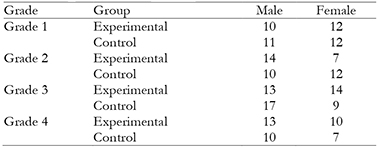
Study included 181 (54.1% male, 45.9% female) Lithuanian primary school students, grades 1-4, consisting of 93 (51.4%) in an experimental group and 88 (48.6%) in a control group. The method used to select the sample was convenience sampling. The participating children ranged in age from 7 to 10 years (Mage = 8.54, SD = 1.10). The number of students in each grade level was approximately the same. The percentages of students in grades 1-4 were 24.9%, 23.8%, 29.3% and 22.1%, respectively. Table 1 presents the distribution of the participants across grade levels and their gender in the experimental and control groups.
Forty five children from the 1st grade (Mage = 7.24, SD = 0.37) were assisted by trained researchers, who were blind to the experimental conditions of the study, with understanding and completing the questionnaire. Children in the other grade levels completed the questionnaire on their own. Written and oral informed consent was obtained from both parent and children in the experimental and control groups. Ethical approval was received from the ethics committee of Lithuanian Sports University.
Measures
The effects of Brain Breaks® were measured by the Attitude toward Physical Activity Scale (Mok et al., 2015). The scale includes a demographic section and eight sub-scales: (a) Physical Fitness measured self-perception of physical fitness (5 items). Example “I am confident with my agility.”, (b) Self-efficacy in using video exercise, measured self-efficacy in using video exercises (4 items). Example “I know how to do physical activity if there is a video exercise to follow.”, (c) Personal Best measured goal orientation in physical activity (4 items). Example “I keep striving for breakthroughs in physical activity.”, (d) Interest measured interests and enjoyment in physical activity (8 items). Example “I enjoy doing physical activity with my classmates.”, (e) Importance of physical activity measured attitudes toward the importance of physical activity (4 items). Example “It is important to spend time to be physically active.”, (f) Benefits of physical activity (4 items). Example “Being physically active helps to give me new experience every time.”, (g) Learning in school subjects, measured contributions of video exercise to learning in school subjects (5 items). Example “I learned about language through video exercise.”, (h) Health, measured contributions of video exercise to health (4 items). Example “I learned about healthy lifestyle from video exercise.”
The scale was internationally validated on a sample comprised of students between grades 1 and 7 in five countries: Lithuania, Poland, Serbia, Singapore and Zimbabwe. It was initially developed in English. Language considerations were accounted by making double back translation. Categorical answers to each question were rated on a scale from 1 to 4 (strongly disagree, disagree, agree and strongly agree), with the higher score reflective of a more positive indicator. Cronbach’s alpha was acceptable, ranging from .629 to .837 in the different sub-scales (Mok et al., 2015).
Procedures
Intervention was carried out in one primary school. Two classes from grades 1-4 participated in the study. For each grade, one class was the experimental group, while the other served as control group. Both groups completed the questionnaires as baseline data. Then, only the experimental classes received the Brain Breaks video exercise intervention every school day in their classrooms during class breaks and supervised by their teachers, with one five- to nine-minute video per day for three months. Each Brain Breaks video provided movement-integrated learning with motor and fitness skills presented by animated and real-life instructors. During the Brain Breaks the children watched the video and also did some exercises following the video instructions. Brain Breaks incorporated health and nutrition education, social learning, environmental stewardship, core curricular learning, character development, arts and culture. The experimental and control groups continued their regularly scheduled physical education for 45 minutes twice weekly. After the intervention, children in both groups repeated the questionnaire.
It should be noted that the video of the Brain Breaks program was not standardized to a fixed interval or time period, because each classroom structure is unique as is the individual teacher or teaching need on any given day. For teachers to use the program routinely and effectively, it needs to be flexible and easily inserted into the varied daily classroom environment. For this reason, teachers have a readily available set of physical activities varying in length to best suit their daily needs. The goal was that teachers used Brain Breaks® routinely and consistently throughout the school day at different moments, such as subject transition, or before and after lunch and recess.
Statistical analysis
The statistical data analysis was completed using SPSS for Windows 19.0 software (SPSS Inc., Chicago, USA). In order to establish factors, EFA was used. The test for data normality using skewness and kurtosis indicated that factors were normally distributed. To analyse the effects of video exercise intervention on APAS scores, one way repeated measure ANOVA with Time and Time x Group (experimental vs. control) within subject factor was used. The children’s gender and age were included in the ANCOVA as covariates. The partial eta-squared (ή²) effect sizes for the tests were calculated to indicate the magnitude of the effect. Magnitude was interpreted as small at the cut-off point of 0.02, medium at the cut-off point of 0.13, and large at the cut-off point of 0.26 (Green, Salkind, & Akey, 1997).
Results
All 181 participants completed both baseline and post-intervention questionnaires. A repeated measure ANOVA with a Greenhouse-Geisser correction determined statistically significant difference of mean scores on Personal Best, F(1, 177) = 6.354, p < 0.05, Interest, F(1, 177) = 4.124, p < 0.05, Importance, F(1, 177) = 5.722, p < 0.05, scales between two time points with both treatment and control groups considered as a composite. Experimental group showed higher scores and control group reported lower scores on these scales at post-intervention comparing to baseline (Table 2).
Table 2: Baseline and post-intervention mean scores adjusted for gender and age, and effect sizes (partial ή²) of differences between time points and between experimental and control group.

Note: *p <.05;**p <.01.
A repeated measure ANOVA with group (experimental vs. control) between subject factor showed significant effect for Time X Group interaction for each scale, indicating differences between treatment and control participants across time. The experimental group reported elevated scores whereas the control group reported lower mean scores for APAS scales, Fitness, F(1, 177) = 79.829, p < 0.05; Self-efficacy, F(1, 177) = 93.813, p < 0.05; Personal Best, F(1, 177) = 48.050, p < 0.05; Interest, F(1, 177) = 50.487, p < 0.05; Importance, F(1, 177) = 50.440, p < 0.05; Benefits, F(1, 177) = 64.530, p < 0.05; Learning, F(1, 177) = 84.486, p < 0.05; Health, F(1, 177) = 122.799, p < 0.05, at post-intervention. Based on the partial ή², magnitude of the effect of Time X Group interaction was the most salient for the scores on Fitness, Self-efficacy, Learning, Benefits and Health, all exceeding partial ή² > .26 (Table 2).
Discussion and Conclusions
This study examined the effect of video exercise intervention program on changes in children’s perceptions, attitudes towards physical activity, physical self-efficacy, health-related and specific academic knowledge acquired.
The results indicated a positive effect of video exercise intervention during breaks measured by a change of APAS scales. In the experimental group, the Brain Breaks® video exercise intervention program improved goal orientation at performing physical activities, increased interest for exercising, perception of importance to exercise regularly, and efforts to perform better in physical activities. Also, at post-intervention, experimental group reported elevated indicators on each APAS scale when compared to the control group. Currently there are a limited number of research examining primary school children’s knowledge, attitudes and beliefs towards PA. Results of a qualitative study has shown that some children possess limited understanding of what constitutes PA (Mackintosh, Knowles, Ridgers, & Fairclough, 2011). Results of the present study revealed that Brain Breaks® intervention aided primary school children’s comprehension regarding the relationship between PA and health, knowledge about health-related behavior, its benefits and self-organization and execution of physical activities, as the experimental group improved most in: understanding how physical activity can promote health, self-efficacy using video for exercising. An additional promising result of the present study was the increase in children’s physical self-confidence, supported by research revealing that children tend to participate in physical activity if they perceive themselves to be physically able, and possess a high degree of confidence and self-efficacy (Mackintosh et al., 2011).
The results of the present study can also be compared with other similar studies involving digital facilities for promoting PA. For instance, PA levels amongst sixth graders were found to be enhanced through the implementation of the Presidential Lifestyle Award program which is comprised of peer leadership and an innovative exercise resource toolkit that includes DVDs (Barr-Anderson et al., 2012). Results from this program intervention were found to be successful in increasing MVPA in children. Both teachers and children reported a high level of receptivity and intrinsic satisfaction with the intervention (Barr-Anderson et al., 2012). As an added inducement to expand the use of digital facilities in PA interventions, the results of a systematic review reveals a potential commitment by digital facilities to produce video games to improve health outcomes (Primack et al., 2012). One example is the Online Streaming Brain Breaks (OLSBB) by HOPSports (2017), referred to as Brain Breaks in this study.
In the current study children in the experimental group improved their educational understanding of academic knowledge: language, art, music, and culture, all interwoven components of this study. This is a very important finding as it shows the potential of education as a continuous process, interchanging curricular education during classes with non-curricular education during recess. Both types of education contribute to a child’s knowledge. This is also in line with contemporary trends and the philosophical concept in education that proposes that PE should be implemented as a wider educational practice instead of being focused only on the body (Emeljanovas, Saulius, & Rutkauskaite, 2014).
The study results conclude that the intervention program through video exercise during breaks in primary school was effective, not only for increasing PA, but also for enabling general education continuity and empowering children to be self-responsible, confident, and competent for their own health and well-being. The systematic literature review of Primack et al. (2012) tested the effect of video games on health and was in line with our results, revealing that video games improved 42% of health education outcomes. The results of the present study prove that the digital facilities, which have increased their popularity worldwide, are an effective way to create cognitive and motivational background for PA in children, resulting in health-enhancing behaviors.
The results of this study clearly support a positive effect of Brain Breaks video exercise on children’s perceptions, attitudes, and knowledge of PA as a health-related behavior. Digital facilities are proven as an effective way to create a cognitive framework for health-enhancing behaviors.
This study is unique for its layered focus not exclusively on PA itself, but on the underlying factors of PA (motivation for exercising, exercise knowledge, physical self-confidence), and specific outcomes such as multidisciplinary primary school curriculum and general knowledge included in the educational content of Brain Breaks videos.
The main limitation of the study is the lack of objectively measured variables. Gathering objective information regarding children’s academic achievement in relation to measured PA levels would be a valuable addition for future studies. Further longitudinal research should consider examining the enduring impact of digitally provided PA on perceptions and change in PA, preferably objectively measured.
A three-month video exercise-training program leads to improvement in children’s attitudes toward physical activity in general, and especially in perception of their physical fitness, self-efficacy, and health-related and specific academic knowledge acquired. It may be concluded that Brain Breaks video exercise intervention program contributes to physical, health and general education of primary school children.

