










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Addictive behaviors represent a complex problem for public health that entails adverse consequences for the individual's personal health and growth, family dynamics, and social development and stability. Talking about addictions refers to a complex, multi-determined behavioral phenomenon that involves diverse factors: genetic, epigenetic, development-related, educational, psychological, environmental, and cultural. This phenomenon is characterized by the creation of new habits or repetitive behaviors that escape brain mechanisms supervising conduct, so that they get repeated because of short-term reinforcement, even if they later cause negative consequences (Lewis, 2015; Volkow, & Baler, 2014).
Addictions have traditionally been associated with substance use, but the characteristics described above can also appear in relation to other specific behaviors, the so-called behavioral addictions (Grant, Potenza, Weinstein, & Gorelick, 2010). Recent research has found evidence that the brain circuits implied in addiction, whether involving substances or not, are essentially the same (Brand, Young, & Laier, 2014; Huang, 2017), which corresponds to previous findings that both conditions share genetic predispositions, personality traits, behavior patterns, and complications in diverse daily-life activities. (Grant, Brewer, & Potenza, 2006).
In recent years, the emergence of smartphones has brought about a new revolution, as it has become the most widely used device for Internet access, largely displacing personal computers. Its easy portability and information accumulation capacity have turned the smartphone into a handheld computer, with unlimited utilities (Pedrero-Pérez, Rodríguez-Monje, & Ruiz-Sánchez de León, 2012).
The limit between use, overuse, and addiction is by no means easy to draw. As previously noted, addiction is currently regarded as a progressing process: from an initial reinforced response, to a habit where some stimulus-response associations prevail that escape the conscious cognitive control (Kuss, & Lopez-Fernandez, 2016). This loss of control makes the individual embrace compulsive, constraining behaviors that can interfere with brain, personal, and social development, and is frequently also associated with mood disorders or other psychopathological expressions (Kaess et al., 2014). Therefore, it is essential to detect risk at initial stages of this process, which would in many cases stop the evolution of the loss of control (Lee, & Lee, 2017), especially in the case of new technologies, which primarily affect subjects with increasingly lower ages (Carbonell et al, 2012) and are linked to the emergence of behaviors derived from high social risk (Arnaiz, Cerezo, Giménez, & Maquilón, 2016).
In order to effectively detect addictions at early stages, it is essential to depend on reliable, validated tools that can be applied in the daily practice of primary care. A study that assesses available resources (Rowan, & Galasso, 2000) suggests that current means are inadequate for clinicians, both for detecting drug consumption and pathological gambling, and that access to quick-to-use, validated, reliable tools would be of major help for their detection, analogously to the CAGE for alcohol-abuse disorders. Following these premises, MULTICAGE CAD-4 (Pedrero-Pérez et al., 2007) was proposed as an initial screening tool for the si-multaneous detection of addictive behaviors involving substances (alcohol and drugs) or not (Internet and videogames addictions, or pathological gambling), as well as other impulse control disorders (eating disorders, compulsive spending, or sex addiction). The MULTICAGE CAD-4 questionnaire, formerly aimed at the population suffering addictions and impulse control disorders, has been later validated for the primary care setting (Rodríguez-Monje, Pedrero-Pérez, Fernández-Girón, Gallardo-Alonso, & Sanz-Cuesta, 2009) and has proven to possess adequate psychometric and diagnostic capacities in both cases. The questionnaire, which is based on the CAGE and follows its 4-question original model, evaluates each of the eight studied addictive disorders, and hence comprises 32 items. A study performed on drug-addicted populations has proven its usefulness for the early diagnosis of these behaviors, allowing for the detection of related addictive behaviors that were neither acknowledged by patients nor identified by the health professionals (Pedrero-Pérez, 2010). Additionally, other studies (Calvo-Francés, 2016; Del Prete et al., 2017; Estevez, Herrero-Fernández, Sarabia, & Jauregui. 2015; Estévez, Ozerinjauregi, Herrero-Fernández, & Jauregui, 2016; Garrido-Elustondo, Reneses, Navalón, Martín, Ramos, & Fuentes, 2016; Jauregui, Estevez, & Urbiola, 2016; Navas et al., 2017; Navas, Verdejo-Garcia, Lopez-Gomez, Maldonado, & Perales, 2016; Pedrero-Pérez et al., 2018; Reneses et al., 201525-32) have shown its utility as a screening tool.
Given the relevance of smartphone overuse and the high prevalence found in several studies (Pedrero-Pérez et al., 2012), it has been decided to include a new scale to assess this problem, which will also allow to complete the profile of addictions to new technologies. The questions included in the smartphone scale follow, as in all other cases, CAGE's basic scheme, asking about the inability to limit the time of use, complaints from significant others about excessive time spent, the need to maintain permanent access to the device and failures in attempts to control behavior. This study aims to assess the adequacy of the psychometric characteristics of the new scale, as well as the preservation of the structural validity of the questionnaire after its inclusion.
Method
Design and procedure
A descriptive, transversal, multicentric study to validate diagnostic tests was conducted in the primary care setting. It was performed in 5 urban primary health care centers, within the public health care system of Madrid, which services a population of 162,461 citizens. The study population comprised subjects older than 14 years who attended primary care consultation for any reason in any of the health centers included in this study and selected by random, non-consecutive sampling. Patients suffering from any moderate to severe mental deficiency or disorder were excluded, as well as those who had problems to read, write, or understand Spanish language. Participants were informed about the study and asked for written consent. In the case of minors, further consent was obtained from their parents or guardians.
The questionnaire was anonymous and self-completed. In addition to the MULTICAGE CAD-4, it recorded the following socio-demographic variables: age, gender, educational level, work status, marital status, access to personal computer, access to videogame console, and social relationships.
A new version of the MULTICAGE CAD-4 was employed which dispensed with the scales regarding eating disorders, compulsive shopping, and sex addiction, and included a new 4-item scale on smartphone overuse. The final questionnaire (ANNEX I) included 24 items from 6 different scales, with 4 questions each that require dichotomous responses (Yes/No), and assess problems involving alcohol consumption, drug abuse, pathological gambling, Internet, videogames, and smartphone use.
Ethical considerations
The protocol for the present study was approved by the Comisión Central de Investigación de la Gerencia de Atención Primaria de Madrid. It has also been approved by the Ethical Committee for Clinical Research of Hospital Universitario Severo Ochoa in Leganes (Madrid).
Data analysis
A descriptive statistical analysis of the variables of inte-rest was performed. The internal consistency of items and scales was studied firstly to assess the questionnaire. Reliability of scales was tested by Standarized Cronbach's. Since the test items are dichotomous and a normal distribution of results is not expected, a confirmatory factor analysis was carried out using the unweighted least squares method. Absolute (χ 2 /df, GFI, RMR), relative (NFI, RFI), and noncentrality-based (PGFI, PNFI) fit indexes were used to test the model. The correlation between the scales was studied by Pearson's r, applying the Bonferroni correction for multiple correlations. FACTOR 10.5 for the reliability, SPSS 22 for correlation and AMOS 21 for the confirmatory and structural analysis were used.
Results
A sample of 2,074 subjects (875 men and 1,199 women) was obtained, with average age 49.7 years (SD=18.7), in a range from 14 to 94. Of them, 5.2% lacked studies, while 31,0% had elementary studies, 15.0% secondary school studies, 13.6% technical training, 14.8% high school studies, and 20.3% university studies. In total, 72.9% had at least one Internet access device for everyday use.
Table 1. Description and internal consistency of items and scales.
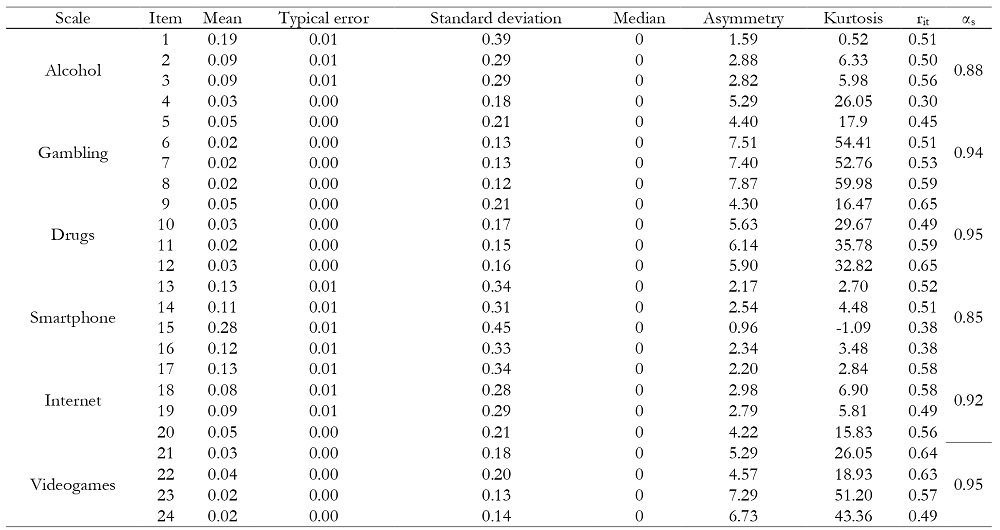
Note: rit= corrected item-test correlation; αs= Standarized Cronbach’s α.
Description and consistency of items of MULTICAGE CAD-4, as well as consistency of the proposed theoretic scales is shown in Table 1, where it can be observed that all scales have a coefficient ( s > 0.85 and all items have a discrimination index r it > 0.30.
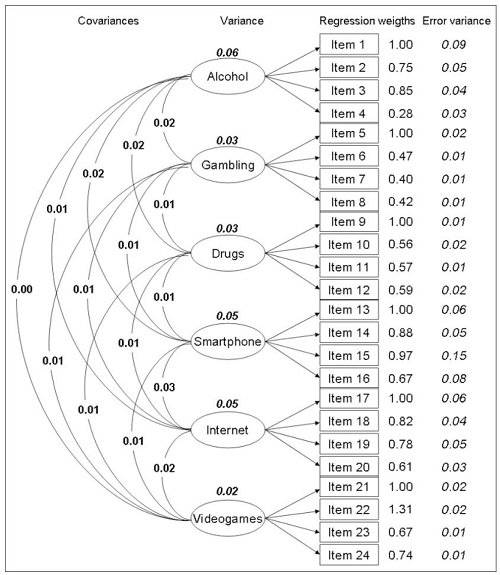
A confirmatory factor analysis was carried out using the unweighted least squares method. An acceptable χ 2 /df= 3.34 was obtained, although it may result from using a very large sample size (n). Absolute adjustment indices were also adequate (GFI=0.99; AGFI=0.98; RMR=0.002) but are also affected by sample size. However, indices not sensitive to size sample were also adequate (NFI=0.97; RFI=0.96), and so were the parsimony ones (PGFI=0.78; PNFI=0.83). The resulting structure is shown in Figure 1.
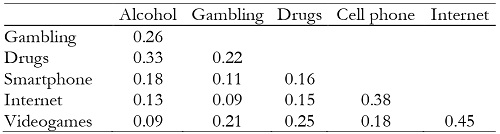
All scales are significantly correlated with each other (Table 2), although the magnitude of the correlations effect varies widely. Maximal correlation is observed between the Internet and videogames scales, Internet and smartphone use, and alcohol and drug abuse.
Discussion
After controlling for the distribution of items, the internal consistency of all the scales was satisfactory, both at the item level and at the complete scales level. The new scale on smartphone use and overuse displayed good internal consistency, analogous to that of the rest of the scales, which supports the high reliability of the whole test.
The outcome of confirmatory factor analysis was fully satisfactory, and all indicators showed an adequate adjustment to the data, especially those not affected by the large sample size. The inclusion of the new scale on smartphone use did not alter the overall structure of the test, which, on the whole, shows a solid structure.
This study has strengths and limitations. Among the first, the use of a non-consecutive sample with an item/subject ratio ˃ 80 allows for applying the most stringent analysis criteria. The age range is very broad, surpassing what is normally included for this type of behavior problems, which is usually limited to samples obtained from young students. As for limitations, the observed evidences of structural validity must be complemented with studies of clinical validity. However, except for pathological gambling, there is a lack of consensus on criteria to determine the degrees of use and overuse in behavioral addictions, and this lack of a gold standard for cut-off points in health practice presents a difficult obstacle to tackle.
This study allows to confirm that MULTICAGE CAD-4 is a quick-to-use, easy-to-answer, robust, and reliable questionnaire with a valid structure to value the presence of dysfunctional behaviors, whether involving substances or not. The inclusion of a scale on problematic smartphone use addresses a current issue of growing worldwide interest, both in the clinical and social realms. The use of screening instruments allows for the early detection of behaviors that can be harmful to the subject, limiting their opportunities for personal development. Just as is the case of other screening tools, it is still necessary to determine its clinical validity, cut-off points, and its sensibility and specificity to detect problematic behaviors. Future studies must draw the limits between normal use, overuse, and dependence on these technologies, find psychopathological correlations between all these addictive behaviors, and define the aims of the research as realistically as possible so that research does not always lag changes in real life.
Conflicts of interests
The authors declare that they have no conflicts of interest.

