










 Servicios personalizados
Servicios personalizados
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
The situations experienced between before, during and after the diagnosis of breast cancer entails a variety of adaptive responses from people that could be connected to medical, socio-cultural and psychological factors , but which in essence constitute a research nucleus of interest, because the efficacy of the treatments established by the survival time and the period of remission is directly related to the quality of life and in close connection with the psychosocial resources that women adopt to face cancer and its treatment (Forjaz and Garrido, 2006).
The discussions that have arisen in recent decades about people's ability to cope have led to the emergence of multiple concepts that range from: problem-focused coping and focusing on emotional consequences (Lazarus and Folkman, 1986); coping focused on the interaction with the obstacle and coping focused on avoidance (Brown and Nicassio, 1987); coping from the dimensions of commitment, separation and seeking help (Osowiecki and Compas, 1999), which are used according to the research needs and theoretical orientation of the authors.
It is interesting to establish the differences between style and coping strategies, first being the predispositions that people use to cope with stress and that allow them to choose between a coping strategy or another; On the other hand, coping strategies constitute a series of behaviors or specific actions to cope with stress that vary according to the contextual conditions among other triggering factors (Pelechano, 2000), however, the theoretical complementarity of both concepts has been demonstrated.
Moos and Schaefer (1993), distinguish coping as a stable disposition of the subject (coping style), or dependent on the contextual factor, giving it a character of transience and concreteness when responding to specific stressful situations (coping strategies).
In this sense, the type of cognitive and behavioral efforts that people use in stressful situations are defined by Lazarus and Folkman (1986) as coping strategies; consequently, coping is determined by the specific situation to be controlled, taking into account that this can be transformed from the learning of various types of activities that people are carrying out according to the need they have.
Coping strategies have been studied in different areas and medical conditions (Lara and Kirchner, 2012, Andrés-Villas, Torrico and Remesal, 2012, De la Fuente, Martínez, Salmerón, Vera and Cardelle-Elawar, 2016); As far as breast cancer is concerned, there are studies that seek to establish the relationship between the risk of having this disease with the performance of screening tests and the possible results that are derived from it, which show according to Cardenal and Cruzado (2014) that coping strategies focused on the problem turn out to be more effective when the woman is at the moment of clarifying a diagnosis of benignity and that screening mammography itself does not generate emotional discomfort for women (Cardenal, Cruzado, González, Rodríguez, González and Valentín, 2013).
For their part, Pieterse, Van Dooren, Seynaeve, Bartels, Rijnsburger and De Koning, (2007), established that the highest levels of anguish are registered by women with breast cancer risks who use passive coping. Therefore, recommendations to the health sector revolves around the strengthening of active coping strategies.
Other studies have explored coping strategies when the woman expects to receive treatment or consultation with the treating oncologist, such as Font and Cardozo (2009) and Henao, Osorio and Parra (2017); who identified that at this time patients diagnosed with breast cancer use different strategies simultaneously that are not exclusive in themselves, and that adaptation and coping in these types of patients occurs in a favorable, integrated and compensatory way (Leyva, Solano, Labrador, Gallegos and Ochoa, 2011) to the extent that women seek balance by enhancing creativity, effort and dedication, that is, employing a range of active coping strategies.
In this direction, there is evidence to suggest that certain strategies and coping styles focused on the problem associated with positive sociodemographic variables are related to a better adjustment to the disease, and therefore produce improvements in the quality of life (Reich and Remor, 2011). A well as in this phase, some studies could establish that the resolution of problems is the most accepted strategies that is related to the type of treatment received, age and the greater schooling among other sociodemographic variables (De Haro, Gallardo, Martínez, Camacho, Velásquez and Paredes, 2014).
Rojas and Varela (2017), focused on analyzing the psychosocial factors associated with the ability to cope in a group of breast cancer survivors, highlighting that women tend to adopt two positions. These are active and passive, with the former focusing on the capacity of empowerment of a series of strategies such as the fighting spirit, self-efficacy that favored the development of their human capacities and that favor the adoption of a resilient, positive and active position that fills them with positivism and allows them to face the processes and achieve survival. Meanwhile the passive is a pessimistic position, assumes a position of resignation and fatality whose line is inscribed with the findings of other research that show a predominance in the style of coping centered on emotion, whose strategies point to dysfunctional processes that increase vulnerability to phenomenon (Montiel, Álvarez and Guerra, 2016).
Optimism related to coping strategies has been a field rich in research in recent decades, some studies that have diagnosed women with breast cancer who are optimistic as usually employ active strategies such as reflection, planning , social support, or sense of humor (Carver, Well, Harris, Noriega, Scheier, Robinson, Ketcham, and Clark, 1993). Other studies suggest that optimistic people tend to adopt active strategies such as adopting a fighting spirit and pessimistic people prefer strategies of hopelessness and helplessness, and these preferences are preserved in the before and after surgery (Schou, Ekeberg, Ruland, 2005).
Dispositional optimism could become a protective factor to mitigate the conditions and effects of the disease, but research results warn that the impact of pessimism is highest in the loss of quality of life of women. Therefore, Instrumental support team has to concentrate their full efforts on strengthening the skills of women to find the tools that allow them to feel emotionally healthy and optimistic (Pujol and Font, 2014).
The experiences of people facing different adversities and situations reveal that not all subjects respond equally to the same stressor, that is, facing the diagnosis of breast cancer. People can react in a different way, on one hand they could assume depressive behavior and isolation from the family and social context; but on the other hand it can generate clinging and attachment behavior and demand more care and affection from their partner, family and friends, possibly taking on the stressful event from three basic dimensions: behavioral, cognitive or emotional.
Therefore, it is necessary to identify the coping strategies used by patients diagnosed with breast cancer treated for mammography at the High Complexity Imaging Diagnostic Center, DIAC SAS, in the city of Montería , Córdoba, Colombia in the period 2013-2017, since the identification and inclusion of this aspect of the psychological and emotional conditions of patients is a necessity in order to guarantee the provision of a service from an integral and quality doctor. It is also important also in order to better understand the psychological reaction that patients assume in relation to this life-threatening disease, in turn obtaining favorable data that help to develop adequate strategies for the treatment of psychic alterations in these patients.
Consequently, the present study was proposed firstly to evaluate the living conditions of the participants based on the reflection of the personal and social characteristics present in women diagnosed with breast cancer; and secondly, it is proposed to analyze the coping styles and strategies of breast cancer patients from the following dimensions: cognitive, affective and behavioral.
Method
Participants
For the execution of the research, the voluntary and anonymous participation of a total of 131 patients diagnosed with breast cancer was taken, who were taken from a total population equivalent to 16,744 patients who were attended and registered in the DIAC SAS database, located in the city of Monteria in the period 2013-2017, in the mammography service, who are affiliated to the subsidized and contributory regime of the General Social Security System in Colombia.
The sample distribution in terms of sex 100% corresponds to women. Participants' ages ranged from 35 to 70 years old (M = 57.23 years, SD = 8.02). All the people who participated in this research were patients diagnosed with breast cancer through mammography. Given the characteristics of the study subjects, none of the patients diagnosed with breast cancer with any screening test other than mammography participated in the study.
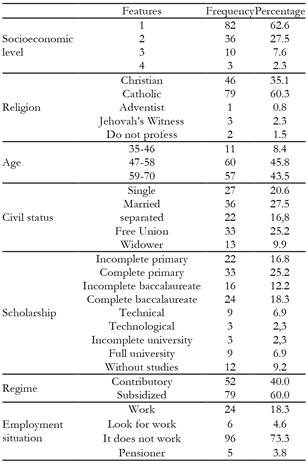
With respect to other sociodemographic data of interest in the study, the sample was distributed in the following way: in relation to its socioeconomic level, the majority of the participants reported living the lowest level (62.6%), with respect to religion 60.3% said they were Catholic and 27.5% were married.
The sample was determined from the total population by simple random sampling. In this case, a probability of success and failure of 50% was estimated, with an error no greater than 5% and a confidence of Zα = 95%.
Instruments
The instruments used were the following:
- Sociodemographic questionnaire: With this questionnaire, information was obtained from the participants regarding their place of residence (central / Alto Sinú / Sinú medio / Bajo Sinú / Alto san Jorge / coastal / Sabana / outside the department); socioeconomic status (1/2/3/4/5/6); religion (Christian / Catholic / Adventist / Jehovah’s witness / other); age (35-46, 47-58, 59-70) ; marital status (single / married / separated / free union / widower); who they live with (parents / couple / children / siblings / single / other); type of housing (owner / family / leased); main contributor to economic sustainability (own resources / family support / couple / government assistance / other); receives special subsidy (yes / no); affiliation to the health system (contributor / beneficiary); regime (contributory, / subsidized); work (works / seeks work / not working / pension); type of contract (indefinite / fixed term / independent / temporary) and schooling (incomplete primary / complete primary / incomplete baccalaureate / complete baccalaureate / technician / technologist / incomplete university / complete university / without studies).
- Inventory Brief- Cope: This instrument was created to evaluate the different responses that people have towards stress, which according to Carver (1997) consists of a multidimensional inventory that is structured from scales whose items conceptually measure aspects related to this event. There are several versions of COPE. However, for studies that address health the Brief-COPE was designed, which is easy to use and is composed of 14 subscales organized into two items, which as a whole value the three domains of the strategies of coping that should be known: cognitive coping, affective coping and behavioral coping, distributed in two coping styles: active and passive.
In the cognitive domain, specifically in the active coping style, positive reformulation, humor and acceptance are evaluated. Meanwhile, in the passive style, negation, religion, use of substances and self-blame are measured. Regarding the emotional domain, the Brief-COPE assesses in the active style the emotional support and the instrumental support, and in the passive style it evaluates the emotional discharge, and in the behavioral domain the evaluation of the active and planning (active style), and the items of renunciation and self-destruction (passive style).
The participants had four options to answer: (1: never, 2: sometimes 3: almost always, 4: always), referring to the frequency with which the person performs an action or develops a type of thinking. High scores indicate a more frequent use of that coping style. On the other hand, the reliability coefficients (internal consistency) of the 14 original subscales have Cronbach's alpha values of between .50 and .90 (Carver, 1997), whose internal consistency turns out to be adequate for this type of study, as well as shows a favorable application in the flexibility of the inventory.
Process
The selection of the sample was carried out randomly, taking into account the selection criteria. The women were given a structured interview, which consisted of two parts, the first where the sociodemographic characteristics were identified, and the second where the Brief-Cope inventory was applied. We had a team of interviewers trained to apply the instrument, which verified that all the fields were answered and there was no missing data.
To determine the level of coping in women diagnosed with breast cancer through mammography, the Estaninos scale was used. Taking into account that coping consists of 14 aforementioned items, the following measurement ranges were considered in coping assessment: bad coping (12 - 24 points), regular coping (24 - 37 points), and good coping (38 - 50 points).
The cognitive category consists of 4 items: planning, positive reformulation, mood and acceptance. The following criteria were considered for the cognitive evaluation: bad coping (4 - 8 points), regular coping (9 - 13 points), and good coping (14 - 18 points). The affective category is evaluated based on emotional support, instrumental support, religion and emotional discharge, and a range was established referring to: bad coping (4 - 8 points), regular coping (9 - 13 points), and good coping (14 - 18 points). Finally, in the behavioral category which consists of 6 items referred to as active coping, resignation, self-distraction, denial, substance use and self-blame, a range of bad coping was considered (6 - 12 points), regular coping (13 - 19 points), and good coping (20 - 24 points).
Data Analysis
Collection and tabulation of the data was performed in Excel 2010 for further analysis using the statistical program SPSS 23.0. A description of the sociodemographic characteristics was made by absolute frequencies and percentages. In relation to the analysis of the coping strategies, the means of the answers were calculated to determine the value of the coping strategies, and the absolute frequencies and percentages were calculated by strategies, by categories and totals. On the other hand, cognitive, affective and behavioral evaluation was determined with descriptive statistics according to established intervals, with tables of two entries classified into categories, strategies and how frequently the strategy was used.
Ethical criteria
The research project from which these results are derived was submitted for evaluation by the Research Ethics Committee of the Faculty of Health Sciences of the University of Córdoba, an entity that verified that ethical risks could be easily determined, and established the valid strategies to be able to control them in the event that they arose throughout the framework of the study.
It was approved by the Ethics Committee for the development of the study and with the endorsement and follow-up of DIAC SAS, based in the city of Monteria, Colombia.
Results
From the application of the sociodemographic questionnaire and its processing with descriptive statistics techniques, absolute frequencies and percentages were obtained that permitted the characterization of the population.
Among the main trends found, it could be established that 62.6% of the participants are from socioeconomic level 1; 60.3% have a Catholic religious affiliation; in the case of age, the participants were grouped in age ranges with 89.3% of the patients being distributed in the groups of 47-58 years and 59-70 years, with atypical participation of a patient of 35 years of age (lower than the recommended for the application of the mammographic test).
Likewise, the main frequency for civil status indicated that 27.5% of the participants were married, 54% had lower educational level and baccalaureate, 76.3% of the patients belonged to the subsidized regime and finally, it was determined that 73% of the participants did not work, figures that can be corroborated in Table 1.
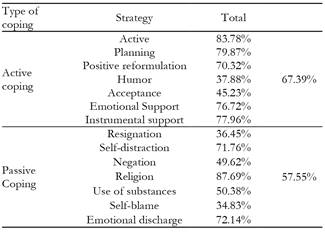
The first classification for the coping strategies used by patients with breast cancer revolved around the attitudinal style of the same, grouped into active and passive, it was found that the main frequency of use was 67.3%, which corresponded to the active ones, while the passive ones had a use of 57% (see Table 2).
Based on the results presented, it is necessary to remember that breast cancer is a stressful event that affects the emotional and psychological stability of patients, so overcoming it requires taking actions and assertive attitudinal decisions within the framework of their coping.
However, according to the classification and grouping of coping strategies these decisions can be organized by their dimension or category, therefore Table 3 shows the frequencies of use for each of the strategies as well as their grouping for cognitive, emotional and behavioral categories.
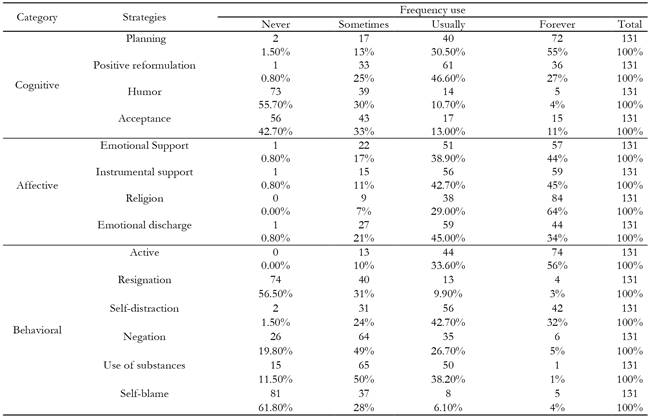
The cognitive category is made up of four coping strategies which were valued by the study subjects as follows: planning (always 55%), positive reframing (usually 46%), humor (never 55%) and acceptance (never 42%). This result shows that patients use planning as the main cognitive coping strategy.
On the other hand, the strategies grouped in the affective category, unlike the other two categories, present the highest level of applicability and use, with religion obtaining the highest frequency of use (29% almost always and 64% always), followed by instrumental support (42.7% almost always and 45% always) and finally emotional support was determined (38.9% almost always, and always 44%).
The behavioral category of coping is made up of 6 strategies. The one with the greatest use in patients being active coping with 56%, while the strategies least implemented by the patients correspond to the self-blame that occupied the main frequency for the option “sometimes” with 28% and “never” with 61.8%, then resignation with 31% for “sometimes” and 61.5% “never”, while the for strategy with the least frequency of use was denial 48% for “sometimes” and 19.8% for “never”.
Table 4 shows some correlations of interest in the present study between the sociodemographic characteristics and the coping strategies used by the participants, identifying that between the relationship d the marital status and the resignation, there was a p value of .005 (< .05). In addition to this, 80.7% of women regardless of their marital status never or only sometimes would use the coping strategy of resignation, and only 13% of the participants would adopt it, where the highest percentage was 8.4% for women who have a partner, whether married or in a free union.
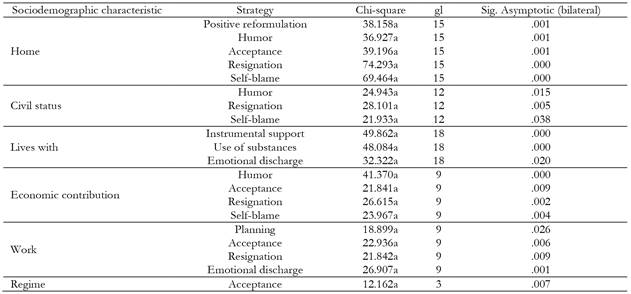
Regarding the relationship between who she currently lives with and the use of instrumental support as a coping strategy for breast cancer, it was found that 95.4% of the women who lived with some type of company, whether it be parents, siblings, partner, children or another relative adopt instrumental support as a coping strategy.
For the relationship between currently living with and the use of substances, a p value of .000 (< .05) was found, and it is evident that 61.1% of women regardless of who they live with never or only sometimes would use substances their as coping strategy, while 38.9% almost always or always would. 16.8% begin the highest percentage and given for those who live with the children.
Regarding humor and economic contribution, a p value of .000 (< .05) was given, and it is related given that 76.3% of the women whose main source was their own resources, and never or only sometimes use humor as a coping strategy.
On the other hand, the relationship between the economic contribution and rejection has a p value 0.002 (<0.05), and a situation similar to that of humor was found, since 74.8% stated that they supported themselves with their own resources and never or only sometimes used resignation as a coping strategy.
Looking at the relationship between economic contribution and self-blame, a p value of .004 (< .05) was obtained. Additionally it was found they that 77.9% of the women who support themselves with their own resources answered that never or only sometimes use self-blame as a coping strategy after the diagnosis of breast cancer, which leads to suppose that those who have their own resources for their support use little rejection.
In short, we found a relationship between the emotional discharge coping strategy and the sociodemographic variable, which indicates a strong association between these two with a p value of .001 (< .05). This can be seen as 73.3 % of women who adopted this emotional discharge strategy do not work.
Discussion
With respect to the first objective, the living conditions evaluated indicate that women diagnosed with breast cancer in the Department of Córdoba, Colombia during the period 2013-2017 present special conditions linked to the social, economic, physical and spatial fragility of the Córdoba territory. According to the National Administrative Department of Statistics (2018), this region poverty index higher than the national average (45.8%), and factors such as being a woman, living in stratum 1, having a low education level, not having a job and belonging to the subsidized regime are interconnected with the appearance of breast cancer.
The behavior of breast cancer, according to the National Institute of Cancerology -INC- (2017), is registered in considering that the disease tends to occur more frequently in regions with better social and economic conditions. This statement that can be corroborated with the results obtained in capital cities such as Bogotá and Cali, where Sánchez, Niño & Estupiñán (2015) and Piñeros, Sánchez, Perry, García, Ocampo and Cendales (2011) detected in Bogotá a population with the majority located in socioeconomic level 3, a better level of schooling, with formal and informal employment and belonging to the contributory regime. For their part, Henao, Osorio & Parra (2017) identified that in the city of Cali, women diagnosed with breast cancer have some education levels (bachelor, technical and university) and the majority are in socioeconomics level 2 and 3.
These results motivate us to investigate what has happened with the health of the women of the Department of Córdoba, who identify with a different behavior in relation to other regions of the country, which offers challenges to public policies that try and address this problem with a differential perspective; more if one takes into account that the economic position of women is a structural barrier that limits access to appropriate treatment, and even affects their ability to receive differential treatment in their care of breast cancer by health care specialistic that affect their ability to cope, because at the same time as suffering from a catastrophic illness they must face discrimination due to their social condition (Sánchez, Laza, Estupiñán & Estupiñán, 2014). Furthermore, according to the results obtained, it can be asserted that unemployed women adopt passive coping styles, specifically the emotional discharge strategy.
Women who have higher levels of schooling are found with better opportunities for early diagnosis and treatment. This could be explained in three ways: the first being the accessibility of tools used in early diagnosis with increasing frequency in clinical testing s and diagnostic tests (INC, 2017), the second is that it maximizes the labor options involving the formal attachment and contributory affiliation of the patient, and finally the level of schooling promotes the adoption of more effective coping strategies that allow them to face and overcome the disease (Sánchez, Laza , Estupiñán & Estupiñán, 2014).
The second objective of this study, planted the idea of the need to analyze the coping styles and strategies used by the participants, but before tackling them, it is necessary make a distinction between these and the style of coping ; In this order, coping styles are the stable or conscious ways that people have to cope with stress, classifying themselves in active confrontation or passive coping.
The findings of this study were able to establish that active coping is the highest frequency used by women diagnosed with breast cancer in the Department of Córdoba. These results are similar to those obtained by Cardenal and Cruzado (2014), who managed to identify that the coping strategies of greater use correspond to the active and problem-centered ones, as well as the findings of Moreno, Gutiérrez and Zayas (2017). These participants opted for active or problem-focused coping mechanisms when they adopted positions of various coping with the problem situation and solving it, although in some opportunities they used styles centered in the handling of the emotions. This moves away from other studies that indicate the adoption of coping styles simultaneously (Henao, Osorio and Parra, 2017; Font and Cardozo, 2009) or in cases where the group of participants uses the same use of styles with the same frequency. oriented towards problem or to the emotion, but they noticed a slight difference with the use of the style oriented to the emotion (Lostaunau, Torrejón and Cassaretto, 2017).
The coping style adopted by the group of participating women becomes positive, because from the perspective of Moreno (2016), people who adopt this is active coping experience better behavior in the face of stress generated from the disease. This is also because they are people that employ positive emotional and psychological attitudes that minimize anxiety (Schou, Ekeberg and Ruland, 2005). Similarly, this type of style makes women with breast cancer diagnosis visible as people motivated by the desire to overcome the disease, understanding it as a challenge to be overcome, especially in a group of women with high levels of social vulnerability, because despite the life conditions recorded by the participants that force them to face that is economic, geographical, labor, administrative, among other barriers, they have a warrior spirit moved by the inner strength that characterizes the Córdoba woman.
The information gathered about coping strategies was analyzed under the theoretical statements that conceive them as a series of specific behaviors that vary according to the context and other triggers; In this regard, the biggest trend was found in the predominance of active coping strategies, which constitutes a key factor in improving the perception of the disease, decreasing psychological distress and improving the quality of life of the patient (Yang , Brothers, and Andersen, 2008). For its part, the results of the use of passive coping strategies, can be understood from associations made from cultural beliefs of breast cancer with death, therefore leading Lazarus and Folkman (1986) to note that passive coping styles arise when the subject feels hopeless before a significant change in the problem or situation that concerns him.
The grouping of the strategies according to their dimension or category of coping was distributed in the cognitive, affective and behavioral dimensions. Regarding the cognitive dimension, the planning strategy obtained the greatest preferences, which could be interpreted as the identification and formulation of the steps to be taken and the direction of the efforts to be made to overcome the disease (Moran and González, 2009). That is to say, the use of this strategy allows us to glimpse the commitment that the patients take in overcoming the disease and looking for the positive side of such a complex situation that they must face.
The strategies within the affective dimension begin with the evaluation of the emotions that the subjects develop before certain events in their lives, and the results show that most of the participants prefer to always use religion, instrumental support and emotional support, and almost always the emotional discharge they have is linked to the fact that Córdoba women profess mostly Catholic religions believe, have a sentimental partner and are mostly surrounded by children, family and friends.
These results are consistent with the level of religiosity that Colombia registers in position 9 among 57 countries that participated in the Gallup International Millennium Survey, obtaining an index of 83%. This is shown in accordance to the results of Hurtado & Finck (2013) who identified that 94% of the participants belong to a religion. Therefore, the Córdoba women hold firm their religious beliefs when facing cancer, which could explain the preference for such a strategy, as well as the findings of Enríquez (2010); García (2007); Delgado, Melgarejo, and Villanueva (2005).
The instrumental and emotional support includes a typology of strategies that are defined as the search for information and help from experts in the field, and the presence of family members, friends and social support networks, respectively (Enríquez, 2010). Living with cancer in company shows a protective factor for the patient, as reflected in the results of the study when it was corroborated that the participants who live with their partner, children, relatives adopt instrumental support and never or only sometimes use the substances as coping. Therefore, women with family and social support manage to identify with greater ease the practices of self-care that they should generate after diagnosis, because from the perspective of Scheneider, Pizzinato and Calderón, 2015 and, Rojas and Varela, 2017, the extent that women are supported allows them to acquire a positive self-perception of themselves, facilitating care.
However, it is necessary to understand that although women receive support from their families and health professionals, the need to reorient public policies that can guarantee better living conditions and the elimination of barriers to health care persists, because the support can only be given if the networks are consolidated, have access to resources, possess relevant information and open new paths for women with a diagnosis of breast cancer, which coincides with the approaches presented by Ojeda and Martínez (2012); Sánchez, Laza, Estupiñán & Estupiñán (2014).
In the behavioral category of coping, the strategy most frequently adopted by patients is active coping, which requires that the participants maintain in constant search for alternatives or ways to overcome the disease this result is related to the fact that participants use self-blame and rejection to a lesser degree; that is to say, women seek alternatives to the problem from their behavioral strategies, but at no time do they allow themselves to be overwhelmed by the situation, which is consistent with the results of Ojeda and Martínez (2012) who identified self-destructive behaviors and distancing as the least used behavioral responses.
Conclusion
The realities of the participants present in this study lofty views of their social conditions, although they do not favor adherence to appropriate life styles that promote their survival. It should be noted that it is not a question of affirming that the socioeconomic stratum, the type of affiliation, or schooling ensure the effectiveness of the cancer treatment because it is clear that this disease has a number of factors acting upon it from other dimensions. What is clear is that having better social conditions promote the opportunity for access to health services, improvements in nutrition, special care, and having the support of their partner and family, as well as having their own resources or employment self-support promotes the adoption of active coping strategies.
Despite the precariousness in the living conditions of the participants, they mostly present an active coping style that allows them to reduce stress levels and improve the perception of the disease, through the constant search for information, the use of positive emotional and psychological attitudes, motivation, self-efficacy and personal control. Among the styles of active coping, the active strategy stood out, while in passive coping, the most widespread tendency was to use religion. Most of the patients surveyed used strategies of affective coping that seeks to lessen the emotional impact of the stressful situation, followed by cognitive coping that tries to look for a meaning to the event, and finally behavioral coping.
For the comprehensive care of patients with breast cancer, the type of coping strategies addressed is an excellent guide to understand the internal implications that subjects must cope with in the context of their disease, and it is necessary to highlight the need to formulate public policies that build on the foundations of psycho-oncology allowing the strengthening of the establishment of coping strategies both active and relevant in order to improve the overall health of patients.
It is important to note that this study presented limitations in terms of the nature of the instruments applied, since it is necessary to address coping strategies in greater depth from the perceptions, emotions and meanings that patients give them. It is also considered as limiting to study the transversality of character that was used for the data collection. Therefore, it is necessary to continue investigating before, during and after the diagnosis to consolidate an integral perspective of the problem in this region of the Colombian Caribbean.

