










 Custom services
Custom services
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Learning difficulties (LD) and their impact on academic achievement (AA) continue to be a major problem in education. Significant numbers of students are found to have some kind of difficulty or delay in one or more academic areas which they cannot overcome, despite the efforts and perseverance of parents and educators. These children are categorized as having Academic or Educational problems (American Psychiatric Association-APA, 2014), since they have AA problems (such as failing exams or having low grades) or poor performance, but the nature and characteristics of their difficulties remain to be determined.
They might fall into the category of Neurodevelopmental Disorders and more specifically, they might be considered to have a Specific Learning Disorder, which is one that occurs during school years and is characterized by persistent difficulties that impede learning the basic academic skills of reading, writing and mathematics (APA, 2014).
A specific diagnosis, however, does not always result from their assessment because the interference that their difficulties cause in academic, social and/or personal areas is insufficient for diagnostic criteria.
Likewise, following the proposals of the APA (2014), Borderline Intellectual Functioning (BIF) or Global Developmental Delay (GDD) could be the cause of the serious difficulties that students have in coping with curricular demands.
On the one hand, BIF is a scientifically accepted category that groups together children with a slow learning pace, nevertheless, at least two aspects must be taken into account for it to be considered as a diagnosis. The first of these is that BIF tends to have similar connotations to those of mild intellectual disability (Artigas-Pallares, Rigau-Ratera & García-Nonell, 2007); however, the two are not the same and distinguishing them requires a careful assessment of intellectual and adaptative functions (APA, 2014). Secondly, as highlighted by Artigas-Pallares & Narvona (2011), it is plausible to believe that a child with low intelligence tends, for example, to pay less attention and, consequently, is more prone to having difficulties in following what is taught. But it is also possible to assume a correlation in the opposite direction, that is to say, that since attention, perception, memory and language are fundamental aspects of intelligence, then if these are affected, there will be negative repercussions on this.
On the other hand, GDD is reserved for children under the age of 5, when they fail to meet expected milestones in various fields of intellectual development or they are too young to take standardized tests, with a re-evaluation being required after a period of time (APA, 2014). As Campos-Castelló (2013) points out, Neurological maturation retardation is not used to label a situation definitively, as it is plausible to assume that there will be a “catch-up”. According to the author, Neurological maturation retardation serves to describe a wide variety of situations in which the working of the nervous system (NS) is altered. It is used to define a transitory situation and if normal maturation is not reached after a certain period of time, its cronopathic character would be substituted by a definitive diagnosis of pathological process.
These two labels - GDD and Neurological maturation retardation - are applied in the early years but need to be re-assessed as the child grows up. Once this has been done, children who are shown to have a neurodevelopmental disorder will be able to receive appropriate psychoeducational treatment, tailored to their particular problems. For those who do not have a neurodevelopmental disorder, the question should be posed as to whether to maintain the diagnosis of developmental delay and whether the children will be guaranteed the support needed to overcome their difficulties.
Early delays develop in very heterogeneous ways. Thus, after the age of five (at which point the label can no longer be used), children can be placed along a continuum of severity which ranges from normotypical development to disability. Children who are affected at an intermediate level, in which certain delays or "neurodevelopmental comparators (difficulties" persist, are placed in the central part of the continuum. Such difficulties are not significantly serious, as they do not meet the diagnostic criteria for neurodevelopmental disorders, but they do interfere considerably with AA and school adaptation and may be responsible for generalised learning difficulties in the school years. It is paramount that the nature and characteristics of these difficulties be determined, since clinical and developmental practice requires clear, precise and differential categories and entities that allow neurodevelopmental diagnoses to be properly constructed.
Bearing this in mind, the aim of this study was to identify which developmental domains are affected in children with maturation retardation and to assess the concept of neurodevelopmental difficulties as a comprehensive construct of generalized learning difficulties.
Method
The search strategy consisted of querying high visibility and impact databases from the fields of Psychology and Medicine: Medline, PsycINFO, WOS, Eric, Dialnet and CSIC, and performing a manual search, over the period of this study, to access material which was not included in electronic databases. The compilation of articles was carried out in the first trimester of 2017 and included articles published between 2006 and March 2017.
In order to identify the largest number of potentially relevant records, the descriptors used were a combination of: (i) terms selected from the controlled vocabulary or thesaurus and (ii) free text-terms. These were applied, initially without filters, in English and in Spanish, both independently and in combination using the operator AND: ((development*; neurodevelopment*) AND (delay; retard*; difficulties; disabilities; dysfunctions; profile; disorders)) and ((”neurocognitive difficulties”; “neurocognitive disabilities”; “neurocognitive dysfunctions”; “neurocognitive disorders”; “neurocognitive profile”) AND (attention; memory; “executive functions”; learning; education; “psychoeducational intervention”; “learning disabilities”)).
Given the high number of records that were returned for the terms “neurodevelopmental disabilities”, “neurodevelopmental disorders”, “neurocognitive disorders” and “developmental delay”, the search period was shortened to between January 2011 and March 2017. Additionally, filters were applied for language (English and Spanish) and age (2-12 years) in PsycINFO and in Medline, and for the categories “Psychology”, “Psychology developmental” and “Neurosciences” in WOS.
Articles were selected in various stages. Firstly the search results were unified and, after eliminating duplicate records by means of the Refworks program, those with clearly irrelevant titles were discarded. Secondly, two researchers evaluated the records which had been selected based on their abstract so as to decide whether the complete article should be consulted, by applying the established inclusion and exclusion criteria. With these results, Kappa was calculated, using the statistics program IBM SPSS version 23, and a concordance index of 0.521 (p < .001) was obtained, which, according to the Landis y Koch Scale (1977) indicates a moderate agreement. The main discrepancies arose from the number of records which one of the researchers considered dubious. This lack of agreement, centred fundamentally on the degree of compliance of some of the inclusion criteria, was resolved in consensus with a third researcher. Finally, the full texts of the potentially relevant articles were retrieved, and these were read critically by the three researchers (separately), in order to apply the established inclusion and exclusion criteria. Queries and disagreements were resolved in group discussions.
In selecting the articles, the criteria for inclusion were that they should focus on childhood and relate to: (i) developmental difficulties and learning difficulties, (ii) LD not included in diagnostic manuals, (iii) a study group without evidence of neurological anomalies, malformations or sensory/motor deficits, (iv) studies on delays in neurodevelopment and LD and (v) studies on the neurocognitive profile of children with developmental difficulties.
We excluded research carried out on adults and on children with: (i) a documented neurological clinical history (including Fetal Alcohol Syndrome), (ii) diagnosis of a major neurodevelopmental disorder, (iii) motor or sensory disability, (iv) genetic alterations or known chromosomal abnormalities and genetic syndromes, as well as hereditary neurological disorders, (v) chronic medical conditions; and those who did not contain evidence which was relevant to the research question or were not empirical studies or original research articles.
For each article, information was extracted on the age range, diagnosis or problem described, the developmental domains affected and their relationship to learning, the existence of comparators (experimental and control group) and the design used. For both the extraction of information and for the bias risk assessment, the Protocol and proposals of the Cochrane Handbook for Systematic Reviews of Intervention (Higgins & Green, 2011) were followed. To evaluate the quality of the articles, A Measurement Tool to Assess Systematic Reviews (AMSTAR) by Shea et al. (2009) was applied and returned a high score (8 out of a maximum of 11 points). The critical domains proposed in the AMSTAR-2 (Shea et al., 2017) were also considered, with five out of seven domains achieving a rating of “yes” or “partially yes”; domains 4 (Risk of bias from individual studies) and 5 (Appropriacy of meta-analytical methods) were not rated. Because of the heterogeneity of the studies, a narrative analysis of the information was performed, according to the outcome variables (limitations in developmental outcomes and learning implications), so there is a possibility of reporting bias.
Results
18 articles were included (see Table 1). The selection process can be seen in Figure 1. The database search yielded 11,027 records, to which 10 manually identified studies were added. After eliminating 10,781 due to duplication and/or the title and another 180 for irrelevant abstracts, 76 articles were selected to be reviewed, with 58 of these eventually being discarded for not meeting the inclusion criteria.

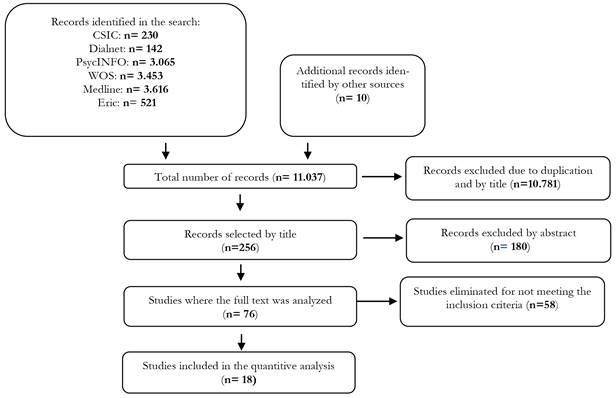
Figure 1. Flow diagram of the process of systematic review. Adaptaded from “Preferred reporting items for systematic reviews and meta-analysis: The PRISMA statement.” by D. Moher, A. Liberati, J. Tetzlaff, D.G., Altman, & The Prisma Group, 2009, PLoS Medicine, 6(6), p. 3.
Generally speaking, the studies fell into four broad types which: (i) focused on major neurodevelopmental disorders that analyzed developmental delays and their relationship with restrictions on activity and participation, (ii) assessed very specific environmental risk factors (urbanity, childhood trauma, etc.), (iii) analyzed exposure to toxins, or (iv) studied the relationship between social disadvantage and specific development problems such as the occurrence of tonic neck reflex, motor skills, etc. Theoretical reviews were also discarded.
The results obtained provided information related to theoretical conceptualization and affected domains and risk contexts - both biological and environmental.
Conceptual approach
“Developmental delay” (DD) or “global developmental delay” (GDD) are the dominant diagnostic labels used in these studies. DD is widely accepted as a general term to characterize children with significant delays in one or more domains when compared with peers, and when this significance usually entails one to two standard deviations below the mean from age-appropriate, standardized and normalized tests (Delgado, Vagi & Scott, 2006, 2007; Perna & Loughan, 2012).
There is however, no consensus on a single definition (Perna & Loughan, 2012) or on specific diagnostic criteria, which vary by country (Delgado et al., 2006). In the USA, although the diagnosis of DD allows children to receive care during the early years (Delgado et al., 2006, 2007), the age range is limited to 5-9 years, depending on the State, and as they mature they must be re-evaluated and labelled with a particular disability in order to receive specialist care (Delgado et al., 2006). Thus, in Florida, the DD diagnosis cannot be applied to children over the age of 5 and so preschoolers who have been diagnosed with DD do not have the same classification as they grow up. (Delgado, 2009). In Brazil, however, children who are born in vulnerable conditions or who have some type of delay in their development process are diagnosed with “global developmental delay” or “neuropsychomotor developmental delay”, as there is no standardized classification, and many of them retain this diagnosis for years even though, it often no longer represents the child’s actual condition (Dornelas et al., 2016).
Research on the outcomes of children who have been identified with DD prior to starting school is sparse (Delgado et al., 2006) and, furthermore, is contradictory in terms of the extent to which delays detected in infancy persist in early childhood (McManus, Robinson & Rosenberg, 2016) or develop into other disorders (Perna & Loughan, 2012). Delgado et al. (2006)’s research supports the idea that the problems inherent in DD are relatively stable. In fact, in their study, the majority of preschool children who were identified as having DD continued to need special education services during their school years. In contrast, the results of McManus et al. (2016), suggest that the problems vary widely and that most are resolved at 24 months. It is possible, as Perna & Loughan, 2012) point out, that some delays are serious and give rise to persistent development problems or brain dysfunctions that manifest differently over time in the development of the nervous system; and some others are mild, in which case these children run the risk of not being identified until they reach school age and, consequently, not receiving early care.
Recent studies indicate that GDD brings together a complex set of symptoms that span a spectrum of several types of problems, with a variety of profiles ranging from children with normal development to those with significant problems (Dornelas, et al., 2016). Greater knowledge about how different domains behave will lead to better judgement as to which children are most at risk for developmental problems (McManus et al., 2016).
Developmental domains: neurodevelopmental functions
Children with DD generally have low AA in the school years and higher grade repetition rates, as Delgado et al. (2006) indicate.
The most affected domains are:
- Cognitive: Several researchers report low mental processing scores (Larroque et al., 2008), worse functioning in the area of cognition (Månsson & Stjernqvist, 2014) or lower IQ in children with developmental delay (Mu, Lin, Chen, Chang & Tsou, 2008; Perna & Loughan, 2012). The cognitive domain is confirmed to be the one with the greatest limitation (De los Reyes-Aragón et al., 2016) and the one in which delays persist more frequently (McManus et al., 2016).
- Attention, memory and executive functions.Potharst et al. (2013) or Perna and Loughan, (2012) report these impaired cognitive functions which, once IQ is controlled, have a significantly lower score in immediate and delayed visual memory skills.
- Communication and language. According to Delgado (2009), 66% of preschool children who were identified as having DD in fourth grade had some disability and, in 77% of cases, this involved problems with speech and/or language. In the same vein, De los Reyes-Aragón et al. (2016) also note delay in communication, Takeuchi et al. (2016) and Potijk, Kerstjens, Bos, Reijneveld, and Winter (2013) report adverse effects on linguistic development, Kerstjens et al. (2011) high rates of impaired scores in communication and Månsson and Stjernqvist (2014) significantly lower scores in receptive and expressive communication.
- Motor, visuospatial and visual-motor skills. Several investigations report general difficulties in motor skills (Dornelas et al., 2016; McManus et al., 2016) or more specifically, in the fine motor domain (Kerstjens et al., 2011; Potijk et al., 2013; Wei et al., 2015), gross (Hsu et al., 2013; Takeuchi et al., 2016), in both (Månsson y Stjernqvist, 2014) or in visual and motor coordination (Potharst et al., 2013).
- Psychosocial and behavioural functioning. Kerstjens et al. (2011) find higher rates of abnormal scores; Potijk et al. (2013) delays in personal and social functioning; Nelson et al. (2016) behavioural difficulties and Takeuchi et al. (2016) challenges in carrying out age-appropriate behaviour.
Biological risks: prematurity and low birth weight
A large body of research, which reports delays in different areas of development, corresponds to studies carried out on preterm and underweight infants.
Hsu et al. (2013) assessed motor and cognitive functions, and the presence of minor neurodevelopmental dysfunctions in 151 children born before the 37th week, at six months of chronologically corrected age. The results highlighted that the lower the gestational age, the higher the likelihood of future neurological developmental difficulties, specifically motor and mental delay.
Månsson & Stjernqvist (2014) studied 399 preterm infants (gestational age <27 weeks) and 366 full term babies. Preterm infants had poorer performance in the areas of cognition, communication (receptive and expressive) and motor skills (fine and gross) at the age of 2.5. In turn, the extremely preterm showed generalized functional deficits at 2.5 years whereas full term babies displayed deficits in specific domains.
Larroque et al. (2008) analysed the neurodevelopment of 2,251 very preterm and extremely preterm children (24-32 weeks of gestation) and of a reference group (born between weeks 39-40). Very preterm births are associated with neurodevelopmental deficiencies at the age of five and the frequency of cerebral palsy, visual deficiency and hearing deficiency and, the mental processing composite decreased as gestational age increased. In general, disability was more frequent in those born at 24-28 weeks than at 29-32 and all degrees of disability decreased as gestational age increased.
Potharst et al. (2013) compared very preterm and full term infants on a wide range of neurocognitive functions at the age of five. Two groups were evaluated: one of 102 infants born before the 30th week and/or with a birth weight less than 1,000 g, and another (control group) of 95 infants born at approximately 37 weeks, with a birth weight of 2,500 g or higher, who attended regular schools. The very preterm obtained poorer scores in processing speed, focused attention, visual-motor coordination and in facial and emotional recognition. As for the executive functions, there was evidence of deficits in the working memory.
Most of the research was centred on very preterm children but, according to Kerstjens et al. (2011), few studies have focused on moderately preterm infants before school age. This research confirms that at preschool age, the prevalence of developmental delay in moderate preterm infants was 2-fold of that in full-term infants and one-half of that in early preterm infants. In preschoolers, the moderately preterm were more likely than full term infants to have fine motor, communication and personal-social functioning problems. In these three domains, the difficulties of the moderately preterm were similar to those of the very preterm, but to a lesser degree. On the other hand, the moderately preterm did not have a higher rate of problems associated with gross motor function or problem-solving when compared with term born babies, whereas the very preterm did. As the authors point out, fine motor impairments may well be the source, at least in part, of writing problems observed in the upper grades; and, secondly, communication difficulties would lead to reading and spelling problems as well as reduced verbal fluency in adulthood. Other studies focus specifically on children with extremely low birth weight (<1,500 g.), and how this fact can lead to difficulties at school age. Mu et al. (2008) evaluated the neonatal findings of children with extremely low birth weight and how this could influence IQ (over or under 90), cognitive function and LD at the ages of six and eight. The children with a lower gestational age had a lower global IQ, but no significant association was found between this and being small for gestational age. Similarly, very low birth weight had little influence on IQ scores at school age. Nevertheless, the authors consider that the difficulties associated with low birth weight persist beyond childhood and that these children may experience cognitive and motor deficits, even if these are not classified as disabilities, as well as slight deficits in intelligence.
The results obtained by Takeuchi et al. (2016) follow the same trend in that they identify low weight for gestational age as a risk factor for DD, even in full term children. When the children were 2.5 years old, information was collected from the parents regarding motor and language development and, when they were 5.5 years old, problems associated with s social development or attention. Low weight for gestational age was found to impact negatively on neurodevelopment (confirming a delay in gross and fine motor development) and on language at the age of 2.5 and, at 5.5 years, on behavioural development (the ability to listen without showing restlessness, to remain patient, to express emotions and to act in a group). These findings contrast, however, with those of Theodore et al. (2009) who analyzed how low birth weight influenced intelligence and which socioeconomic, postnatal, and pregnancy factors were associated with general intelligence at age seven. Children with adequate weight obtained a higher overall IQ score, although the differences were only marginally significant and disappeared when the other factors under study were controlled. A low IQ was found, however, to have a significant correlation with reduced parental schooling, the act of having experienced DD at the age of one and not being the firstborn.
Environmental risk: contextual characteristics
The results of Potijk et al. (2013) show that moderate prematurity and low socio-economic status are separate risk factors with multiplying effects on DD in early childhood. In China, research carried out by Wei et al. (2015) revealed a high prevalence (40%) of DD in children under the age of three in poor, rural areas. The children who lived in poor families, were deprived of learning materials and activities, and whose carers suffered depression were more likely to have delays in neurological development, especially in motor skills (21.4% fine and 18.5% gross) and in problem-solving (18.4%). Higher family incomes were a potential protective factor for child development.
The study by De los Reyes-Aragón et al. (2016) in rural and low-income municipalities in Colombia follows the same line. Widespread developmental delay was found to have 17% prevalence, with the most affected domains being cognitive (35.5%) and communication (21.5%). Furthermore, when analysing the development of delays over time, they found that they worsened with age, especially in the two most affected domains (cognition and language).
Nelson et al. (2016) defined, on a nationwide scale, the large population of young children who were probably not eligible for an educational intervention but were nevertheless at high risk of having poor cognitive and behavioural outcomes upon entering nursery school. The aim was to validate two models: one of academic risk and the other of behavioural risk. The results indicated that both models had the following risk predictors: higher level of education, parents' health status, frequency of reading with the child at home and food insecurity. Finally, McManus et al. (2016) analyzed the permanence, at two years of age, of DD identified at nine months. Social variables such as the caregiver's education, employment and occupation data were important predictors of cognitive DD. This highlights the need to develop eligibility criteria that take into account social variables when identifying children who are likely to need early intervention services.
Discussion
The results reveal: that “Developmental delay” or, less frequently, “Generalised Developmental Delay” are the diagnostic labels which bring together research that focuses on the difficulties or limitations presented by children with regard to developmental domains; that in most countries, these categories are only applied to young children; that there is a lack of consensus on a single definition; that the target population is preterm and underweight children and (to a lesser extent but with growing interest) children who grow up in less-favoured environments; and, finally that the developmental domains which are especially affected are: cognition, attention, memory, executive functions, communication and language, motor skills, visuospatial and visual-motor skills and psychosocial and behavioural functioning.
The definition of DD, as a below-average rate of development, is intuitive but also imprecise. This concept needs to be made operational but, as Aylward (2009) points out, this is no simple task. Proof of this is that, for example, in the USA, depending on the State, more than 20 different definitions of delay are used to determine eligibility for early intervention services (Rosenberg, Robinson, Shaw & Ellison, 2013).
The diagnosis of DD provides a viable solution for children with nonspecific delays who do not meet the criteria for the more traditional disability categories (Delgado et al., 2006) and allows for care to be given during the early years (Delgado et al., 2007). Its identification and early intervention can improve areas of weakness and, perhaps, reduce the risk of subsequent diagnoses (Perna & Loughan, 2012). Nonetheless, limiting the age range to 5-9 years entails that in order to receive special attention as they mature, they must be reassessed and labelled with a particular disability (Delgado et al., 2006). The majority continue to require special education services (Delgado et al., 2006) and some are re-classified, with the most common categories being: specific learning disabilities, speech or language impairment and educable mental handicap (Bernheimer, Keogh & Coots, 1993; Delgado et al. 2006; Keogh, Coots & Bernheimer, 1996). Others, however, do not match diagnostic categories, which leads to their problems being minimized and a lack of provision of adequate care, even though throughout their childhood they demonstrate less readiness for school and are at a greater risk of poor school performance (Montes, Lotyczewski, Halterman, & Hightower, 2012; Romano, Babchishin, Pagani & Kohen, 2010), as well as having deficits in activity, poorer adaptation and decreased participation in school (Leung, Chan, Chung & Pang, 2011). Therefore, both the children identified in childhood with DD (but who do not meet the criteria for a neurodevelopmental disorder to be diagnosed in later years) and those who at school age are given an imprecise diagnosis such as being immature, absent-minded or even lazy, must be assumed to have developmental problems that interfere with their learning and must be assigned to a diagnostic category in order to provide them with treatment that meets their needs.
DD in the early years is associated with limitations in cognition, attention, memory, executive functions, communication and language, motor skills, visuospatial and visual-motor skills, and psychosocial and behavioural functioning. These difficulties are related to neurodevelopmental functions that can be considered responsible for the children's low academic performance and problems with adapting to school, and, as Masten et al., (2004) point out, should be considered independently but also holistically, as delay in one domain often has cascading effects on other areas of child health and development, with long-lasting repercussions on AA, health and future opportunities (Obradovic, Burt, & Masten, 2010; Shonkoff, 2011). Despite this, the plasticity of the infantile brain is widely acknowledged and a neuroconstructivist approach should be adopted.
Neuropsychological approaches suggest that deficits at a basic level directly affect one or more "modules" but have little impact on the rest of the system; in contrast, a neuroconstructivist approach assumes that deficits at a basic level have cascading effects that alter interactions within and between networks (D´Souza & Karniloff-Smith, 2017). Neuroconstructivism therefore calls for researchers to adopt a specifically developmental approach, which revolves around change over time, in order to understand the interactions between the genetic, cellular, neuronal, cognitive, behavioural and environmental levels of description of development and its alterations.
This is critical to discovering how an initial change in one domain and at one level of analysis can, over time, influence the others.
An integrative and multidimensional approach must also be adopted in the understanding of the aetiology of DD. In addition to the risk factors for DD in childhood which derive from biological fragilities, such as prematurity or low birth weight, (Ballantyne, Benzies, McDonald, Magill-Evans & Tough, 2016; Sansavini, Guarini & Savini, 2011; Spittle et al., 2017), environmental factors must also be taken into account, such as low parental education (Charkaluk et al., 2017; Hillemeier, Morgan, Farkas & Maczuga, 2011), the lack of a family structure (Kayrouz, Milne & McDonald, 2017), monthly income (Hillemeier et al., 2011) and the number of children (Ozkan, Senel, Arslan & Karacan, 2012) or, in general, child poverty (Dickerson & Popli, 2016; Najman et al., 2009). In fact, as Wei et al. (2015) point out, these factors are associated with adverse experiences at an early age, such as inadequate stimulation or excessive stress, and exposure to multiple risks which affect brain development. Similarly, households with more opportunities and stimulants are linked to better motor and cognitive development (Miquelote, Santos, Caçola, Montebelo & Gabbard, 2012).
For this reason, McManus et al. (2016) suggest the procedures for identifying the children who will have or will develop persistent delays could be improved by the use of demographic information about the family. This is especially relevant if, as Pereira, Valentini & Saccani (2016) point out, although different factors can influence child development, in the long term environmental factors prevail over individual factors.
Conclusions
This systematic review helps to demarcate what DD and GDD are, as well as, in the case of DD, to clarify its aetiology and to specify which neurodevelopmental functions are involved, thereby allowing its repercussions on learning difficulties to be analyzed.
The results are important for three reasons. In first place, given the importance of identifying these children early on so as to avoid or mitigate adverse effects on development and learning, they demonstrate the need for their evaluation as a diagnostic category not only in infancy but also in childhood, throughout their years of primary schooling. Secondly, they underline the need to work on neurodevelopmental functions as basic tools for learning in the field of psychoeducational intervention and to adopt a neuroconstructivist model as a framework, challenging current paradigms that focus exclusively on intervention in particular processes. Finally, they assess the impact not only of biological factors but also of characteristics and variables relating to the family for their medium- and long-term consequences.
The association between neurodevelopmental difficulties and general learning difficulties and their continuation in childhood are highlighted as implications, pointing to the former as an explanatory construct of the latter. The concept of neurodevelopmental difficulties would encompass a broad spectrum of deficits with different degrees of severity that, when interacting with each other, give rise to a variety of profiles. Regarding limitations, we should mention that on one level (that of study) there is a "reporting bias", as we report, selectively, on research that analyzes the impact on learning of children with developmental delay. At another level (that of review), the studies used focus on at-risk populations, there have been no retrospective studies linking LD to developmental limitations, and few studies looking at medium and long-term implications in children with DD not included in the category of disorders.
Finally, understanding the prevalence of this problem will help professionals to anticipate likely or potential difficulties, to develop expectations, to communicate information to parents and educators, and to plan and manage resources to provide care measures tailored to the needs of these children. All this may imply the need for further training, hence the need for future research with large samples so as to better understand the stability and nature of deficits and assess their effectiveness as a diagnostic category.

