










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Noncommunicable diseases (NCDs), also called chronic diseases, are usually a longstanding health problem derived from a combination of genetic, physiological, environmental, and behavioral factors (World Health Organization, 2018). NCDs have rapidly grown in the last years globally because of population aging and the diffusion of unhealthy behaviors (Chen, Kuhn, Prettner, & Bloom, 2018). The consequent rise of the rate of workers with NCDs has been leading to a substantial socio-economic burden in industrialized countries that could rise substantially over the coming decades (Bloom et al., 2011). In Mexico, a loss of 6.3% of gross domestic product is forecasted by 2030 due to health issues in the working population (Asociación Mexicana de Industrias de Investigación Farmacéutica A.C., 2016).
People working with chronic diseases have more sick leaves and long-term work disability (Bergh, Baigi, Mansson, Mattsson, & Marklund, 2007; Roskes, Donders, & Van Der Gulden, 2005), carrying society-level consequences, such as high disability costs and loss of skills and experience for the labor force (Boot et al., 2013).
To reduce the economic, societal, and personal costs associated with NCDs, it is essential to facilitate the return to work (RTW) of workers with acquired NCDs and promote their sustainable job retention. For these workers, it is crucial to have a good quality of working life that allows them to take care of their health and being productive at the same time (de Jong et al., 2015; Miglioretti & Gragnano, 2016). Researchers have investigated factors related to job retention of workers with NCDs (Young, 2010).
The concept of Work-health balance (WHB) has been developed from this literature together with its measuring instrument, the work-health balance questionnaire (WHBq) (Gragnano et al., 2017). The WHB states that sustainable job retention is possible, especially for workers with NCDs and elderly workers, when the worker feels able to effectively balance health and work needs. The feeling arises from the balancing between the perception of how much the characteristics of one's work are barriers to health needs and the evaluation of the helpfulness of the working environment to meet health needs. Preliminary results supported the usefulness of the WHB concept (Gragnano et al., 2017). WHB is more challenging to attain for workers with NCDs than those without (Gragnano, Previtali, Manzi, & Miglioretti, 2018). Moreover, workers with cardiovascular diseases needed less time to RTW with a higher level of WHB (Massimo Miglioretti, Federica, Manzi, & Gragnano, 2019). A good WHB was associated with higher job autonomy, engagement, and satisfaction whereas a low level of WHB was associated with higher levels of absenteeism, emotional exhaustion, workaholism, and general psychological distress (Gragnano et al., 2017, 2018; Previtali, Gragnano, & Miglioretti, 2018). Finally, the WHB explained more of the variance in job satisfaction than the work-family balance in a sample of 318 workers (Gragnano, Simbula, & Miglioretti, 2020).
The WHBq is a useful instrument to understand the work experience of people with NCDs and what needs to change to allow them a healthy work involvement. Employers struggling to maintain a high level of productivity in the face of an increasing population of workers with NCDs could benefit from the information derived from the WHBq.
The WHBq was originally developed in the Italian language. Good psychometric properties of the WHBq were demonstrated with exploratory and confirmatory factor analysis, as well as Rasch analyses (Gragnano et al., 2017; Massimo Miglioretti & Gragnano, 2017). Results of a confirmatory factor analysis with a sample of 525 workers supported the three factorial structure in its original Italian version (Gragnano et al., 2017). However, there are no validated translations published in the Spanish language. A validated Spanish version of the WHBq would be very useful, particularly, for Mexico's context.
In 2016, NCDs accounted for 80% of all deaths in Mexico. The prevalence of many of these diseases increases with age and with the presence of cardiometabolic risk factors (Alwan, 2011; Leitner et al., 2017; Schellevis, 2013).
Concerning aging, in Mexico, the population of 65-year-old adults and older is projected to change from 6.9 in 2016 to 16.8 percent of the total population by 2050 (Muradás, Gutiérrez, & Téllez, 2018). Regarding cardiometabolic risk factors, between 2018 and 2019, the Mexican population had a prevalence of obesity of 36.1% among adults aged 20 years or older, 34.1% had arterial hypertension and 10.3% had a diagnosis of diabetes (Shamah-Levy, T et al., 2020).
The present study aimed to translate and adapt the WHBq into Spanish and to provide evidence for its factorial structure, reliability, and validity. This will be done by replicating the original factor structure of WHBq, testing factor validity and reliability, and investigating concurrent and differential validity analyzing the relationships with external criteria. Specifically, following the rationale that WHB becomes more relevant for workers with NCDs and elderly workers (Gragnano et al., 2017), we hypothesized that as age increases, as well as with the presence of disease, health needs arise, making it harder to cope with job demands, thus making the WHB more difficult.
Hypothesis 1: Workers with a disease have a significantly lower level of WHB than healthy workers.
Hypothesis 2: The WHB correlates negatively with workers’ age.
We also expected commuting time to work to be related to WHB since longer commutes reduce the time for other activities needed to preserve and promote health, and we expected the same would happen with work hours.
Hypothesis 3: The WHB correlates negatively with commuting time to work.
Hypothesis 4: The WHB correlates negatively with work hours.
We also expected work shift to be related to WHB index. Because working in the evening and night is associate with more health problems (Jørgensen, Karlsen, Stayner, Hansen, & Andersen, 2017; Zhao et al., 2019), the WHB is more challenging to attain for workers with the evening shift compared to those on other shifts.
Hypothesis 5: The level of WHB is lower for workers with the evening shift or shift work.
Finally, theoretically, the WHB assumes that the balancing act between men and women is the same.
Hypothesis 6: The average level of WHB across gender is not significantly different.
Method
Participants and procedure
The first part of the study consisted of the translation of the original instrument into Spanish and a questionnaire pre-test that involved a convenience sample of 39 workers, namely, 36 office workers laboring in a school and three security guards from different school grades, with an age range of 30 - 60 years old.
In the second part of the study, the psychometric properties of the final version of Spanish WHBq were tested. The estimated required sample size was 300 based on simulation studies with a similar three-factorial model with around 17 indicators and considering limited model misspecification (MacCallum, Widaman, Preacher, & Hong, 2001; Wolf, Harrington, Clark, & Miller, 2013).
A convenience sampling technique was employed to recruit the workers. The internet-based survey was developed using Google Forms and was shared with the researchers’ contact list. This kind of survey allows for greater heterogeneity in the type of jobs included in the study.
Studies have supported the hypothesis that the validity and reliability of web-based surveys are comparable to those obtained by other classic methods and self-reports (Liao & Hsieh, 2017; Ritter, Lorig, Laurent, & Matthews, 2004).
For this web-based survey, an electronic informed consent form was included previously to the instrument, consisting of a brief explanation of the research, assuring them of anonymity. If the person accepted to participate, the questionnaire was displayed. This investigation was approved by the Ethics Committee of the International Association of Doctors and Health Sciences at Work (ref: AIDCST - 10 - 2019).
The questionnaire was sent online to literate workers 18 years or older that had agreed to participate in the study, and that could use a computer or a smartphone to access the questionnaire. The questionnaire included a section of sociodemographic characteristics, including occupation, sex, age, work shift, work hours, commuting time, and the presence of a current disease. Workers were from the following occupations: administrative work (121, 43.4%), education (51, 18.3%), health worker (24, 8.6%), manufacture (24, 8.6%), salesmen (22, 7.9%) and other (37, 13.2%), accounting for 279 workers. Most of the workers were female (170, 61%), and the mean age of the sample was 35.3 years old (SD 11.3). The main work shift was working in the morning (229; 82%) and most of the workers reported not having any disease (227, 86%).
In the end, the sample to analyze reliability and CFA consisted of 316 workers, that is, 39 from the pre-test (since there were no substantial changes in the questionnaire), and 277 from the survey, since 2 questionnaires were excluded due to missing data.
WHB Questionnaire
The questionnaire comprised 17 items that identified 3 factors. These were Work-Health Incompatibility (WHI, 6 items) and External Support (ES, 6 items) with a 5-point response scale from 1 (Never) to 5 (Always), and Health Climate (HC, 5 items) with a 5-point response scale from 1 (Strongly disagree) to 5 (Strongly agree) (Gragnano et al., 2017). WHI is a measure of how much the worker perceives the present job as an obstacle to the management of his/her health needs, and it is a consequence of the evaluation of the personal abilities to manage the situation, of the present work situation, and the health requests. ES indicates the perceived degree of work flexibility and supervisor support for health reasons. Finally, HC measures how much management behavior is perceived as genuinely interested in the employees’ health. The score of every dimension is the mean value of the items. The WHB index derives from the formula: (ES + HC)/2 - WHI, after the score of every dimension is standardized in T-scores. It can range from - 80 to + 80. In the WHB index, the perception of how much the working environment is favorably disposed toward personal health needs is counterbalanced with the perception of incompatibility between work and health.
Translation Procedure and Cultural Adaptation
The WHBq was adapted, for the most part, using the Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures involving a ‘forward-backward’ translation method (Beaton, Bombardier, Guillemin, & Ferraz, 2000). At first, one of the developers of the original questionnaire shared with the other authors a clear explanation of the construct to avoid any misinterpretation during the translation process.
For the second stage, an initial translation was made from the instrument in the original language (Italian) into the target language (Spanish) by two Spanish native speakers who were health professionals with knowledge of Italian, without any previous information about the instrument's aim nor the construct.
In the third stage, these two translations were reviewed and discussed to make a synthesis into one translation. The team employed for this was composed of one occupational psychologist, a medical doctor, two public health professionals, and a Spanish language professional. At this point, each item and term were analyzed to see if they were sufficiently clear and fit the workers’ context in Mexico.
At the fourth stage, a back-translation was made from Spanish to Italian by a bilingual Italian professional translator, without any knowledge of the original scale. Afterward, this translation was discussed with one of the authors of the original questionnaire, and he issued recommendations to make suitable changes to achieve semantic equivalence.
At the fifth stage, we conducted a pre-test of the instrument in the target language to assess the clarity of the items and wording, with a convenience sample of 39 people, namely, 36 office workers and three security guards from different school grades. These workers were asked to give feedback on the questionnaire as pertains to clarity and wording of the items or express any doubt or ambiguous questions. The issue raised by some workers was about the use of the Spanish word for boss, as it can refer to a supervisor or a manager. In order to clarify this, we asked one of the authors what the original intention was, and he explained that it referred to the immediate boss, and then we modified the items accordingly.
Statistical and Psychometric Analyses
Initially, we calculated the absolute kurtosis and skewness values of the WHBq items to test for deviations from the normal distribution. All values were lower than |2.00|, indicating negligible problems (Bandalos, Finney, & Finney, 2018).
To test the factor validity of the Spanish WHBq, we performed confirmatory factor analyses fitting a three-factor model with latent factors free to covary as the original Italian version of the WHBq. Because our data were approximately normally distributed, and responses were given on a five-point scale, we used the maximum likelihood (ML) estimator (Finney & DiStefano, 2013).
We reported the standardized factor loadings and the goodness-of-fit of the models with the χ2 statistic, the RMSEA (root mean square error of approximation), the CFI (comparative fit index), and the SRMR (standardized root mean square residual). We considered the model fit to be acceptable when RMSEA ≤ .08, CFI ≥ 0.95, and SRMR ≤ .07 (Bagozzi & Yi, 2012; Lai & Green, 2016), with all factor loadings statistically significant. In case of low fit of the model, modification indexes were inspected to understand if meaningful modifications could substantially increase the fit of the model. Competitor non-nested models were compared with Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) with lower values indicating a better fit.
Besides evaluating the global fit of the model, we evaluated the convergent and discriminant validity of latent variables. Reliability was measured with ω (omega) and the average variance extracted (AVE). The estimation of ω assumes the factor model is congeneric - items of the same latent variable can have different factor loadings, whereas the first assumes Tau-equivalence - all factor loadings are equal. The value of ω should be higher than .60, ideally higher than .70 (Dunn, Baguley, & Brunsden, 2014; Field, Miles, & Field, 2012). The AVE measures the level of variance captured by a construct compared to the level due to measurement error. AVE should be equal to or higher than .50. An AVE lower than .50 indicates the variance due to measurement error is greater than the variance depicted by the construct (Hair, Anderson, Tatham, & Black, 1998). All these analyses were performed in R (R Core Team, 2018).
To analyze concurrent and differential validity, we tested the hypotheses about the correlation of the WHB index with external variables. We estimated Spearman’s correlation when the external variable was continuous and Mann-Whitney U when the external variable was categorical because the normality assumption was not met. With the other variables, we performed an ANOVA when the external variable was categorical, in this last case we used Levene’s test to confirm the homogeneity of variance when the p - value >0.05. The threshold for statistical significance was set at <0.05. These analyses were performed using IBM SPSS Statistics 22 (IBM Corp, 2013).
Results
Factor validity
The confirmatory factor analysis was conducted using the lavaan package v. 0.6-4 for R (Rosseel, 2012).
The first model matched the theoretical factorial structure of the questionnaire. Three factors loaded on 17 items: Work-Health Incompatibility (WHI, items 1 - 6), Health Climate (HC, items 7 - 11), and External Support (ES, items 12 - 17). All latent variables were free to covary.
As shown in Table 1, the fit of the first model was not satisfactory. The inspection of modification indexes suggested to free covariance between the errors of items 16 - “Your supervisor listens when you talk about your health” and 17 - “Your supervisor acknowledges that you may have specific needs for your health status”. This modification could be made under the rationale that the last two questions of ES are both related to the supervisor, and their meaning is more similar compared to one of the other items in the subscale ES. The second model was the same as the first one but with a covariance between the errors of items 16 and 17. The model fit improved but did not reach a satisfactory fit as presented in Table 1.
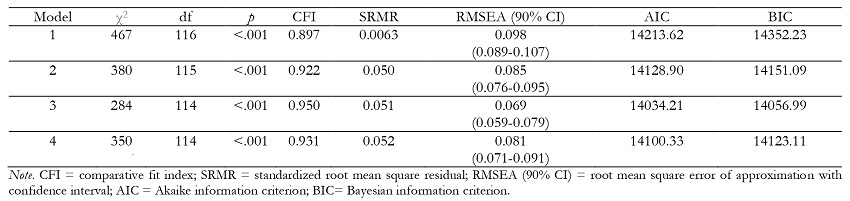
Once more, modification indices suggested to free covariance between the error of items 7 - “Senior management acts decisively when concerns about health emerge between employees”, and 8 - “Senior management considers employee health to be as important as productivity”. This modification could be made under the rationale that these two items are more abstract than the rest of the items in the subscale HC. Model 3 was the same as Model 2 but with a covariance between the errors of items 7 and 8. Table 1 displays the fit of Model 3 that was satisfactory. In this model, the two measures of the perception of how much the working environment is favorably disposed toward the personal health needs - HC and ES - had a significant positive correlation of .75. These measures correlated significantly but negatively with WHI, the perception of the job as an obstacle to the management of health needs (correlations between WHI and HC of -.46; correlation between WHI and ES of -.50).
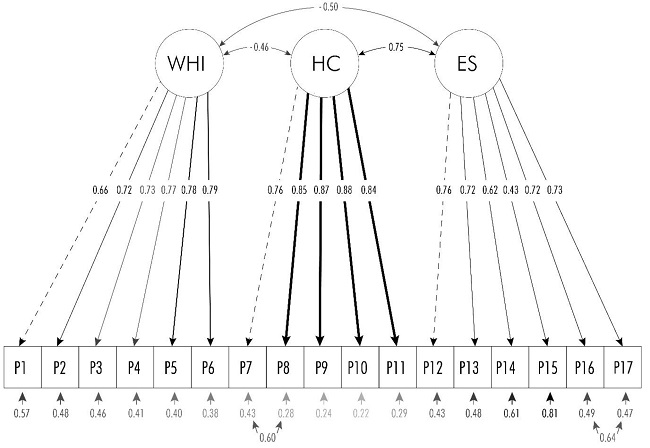
In the CFA with the Italian version of the WHBq, the estimated covariances between item errors were between items 16 and 17, as in Model 2 and 3, and between items 3 and 4, instead of items 7 and 8 as we did in Model 3. Therefore, Model 4 was estimated to reproduce the model fitted with the Italian sample fixing in Model 3 the covariance between the errors of items 7 and 8 and freeing the covariance between the errors of items 3 and 4. Table 1 shows the fit of Model 4. The CFI level was slightly lower than required, and the RMSEA was slightly higher. Moreover, AIC and BIC were better in Model 3. Thus, we concluded that Model 3 was the best. All factor loadings were statistically significant in every one of the models tested. Figure 1 presents the three-factorial structure of Model 3 with standardized parameters. The figure was created using the semPlot package (Epskamp, Stuber, Nak, Veenman, & Jorgensen, 2019).
Reliability
To evaluate internal consistency, ω and AVE were calculated using semTools package (Jorgensen, Pornprasermanit, Schoemann, & Roseel, 2019). The ω coefficient of the whole questionnaire was .84. Model 3 presented ω values higher than .70, but AVE was lower than .50 in the dimension ES (Table 2).

The estimates of the factor ES in Model 3 (Figure 1) showed a factor loading and a measurement error of item 15 respectively much lower and higher than those of the other items. A visual inspection of items distribution of ES (Figure 2) showed a markedly different behavior of participants when they answered item 15 compared to the others.

Concurrent and differential validity
Some additional data were analyzed to screen for correlations using the final model. Rho spearman was calculated, correlating age, work hours, and commuting time to work with the Work-Health Balance Index, namely, the total score of the questionnaire. Table 3 shows the results of the correlations. Two correlations were statistically significant. Age and commuting time to work was negatively correlated with the WHB Index. These correlations indicate that as age and commuting time to work increased, the WHB Index decreased. The correlation between the work hours and the WHB index was not statistically significant. In addition, we compared the means of the total scores with some sample characteristics, as they are seen in Table 4. Two group differences were significant. First, workers that reported having a disease had a mean WHB index significantly lower than those that did not report a current disease. Second, there was a significant difference in the WHB index of workers with different work shifts. Nevertheless, the WHB index did not differ significantly between male and female workers.


Discussion
The study aimed to translate, adapt, and validate the Work-Health Balance questionnaire into Spanish. The findings show that after adapting the questionnaire, it was well understood by workers in this population. The results are consistent in showing the reliability and validity of the Spanish version of the WHBq.
The CFA substantially replicated the three-factor structure of the original questionnaire, supporting the factor validity of the Spanish questionnaire. However, it also highlighted a difference consisting in the estimate of the covariance between the errors of items 7 and 8, instead of items 3 and 4 as in the CFA of the original questionnaire. This difference does not constitute a problem in the practical use of the questionnaire and could be due to differences between the samples of the two countries.
Regarding the standardized solution of the final model (Model 3), it is worth noting that the correlations between WHI and ES, WHI and HC, and HC and ES, are significant, but not close to one, suggesting that even if they are related, they are different dimensions. The correlation between HC and ES is higher than those of WHI with HC and ES as theoretically expected.
The reliability of the dimensions of the WHBq was satisfactory, in terms of ω and AVE for all the subscales except for ES. The AVE of ES was lower than .50 because of item 15. Item 15 introduced in the scale more measurement error than the variance explained indicating the need for further examination. Item 15 states, “It is O.K. with your supervisor if you work at home for health reasons?” Further investigation and sample comparisons should clarify the issue. For the moment, it is advised to keep the same number of items in the Spanish WHBq as in the original version given ω was good and factor loading was acceptable (.43).
The test of the hypotheses provides support to the concurrent and differential validity of the WHB, substantially confirming theoretically expected relation with external variables. The results show that there was a significant inverse association of Work-Health Balance with age, which supports the hypothesis that health needs that increase with age could be hampering the balancing act between work and health. As for commuting time to work, the findings suggest that longer commutes could be affecting WHB, probably by reducing time employed for health (Milner, Badland, Kavanagh, & LaMontagne, 2017). We hypothesized the same would happen with work hours, but we did not find a significant relationship, this has to be studied further since this variable has been related to many health outcomes (Bannai & Tamakoshi, 2014).
The difference in the level of WHB was not significant across gender, which suggests that the same balancing act proposed by the theory is alike in this population. However, workers with diseases had a significantly lower level of WHB than healthy workers, and workers with the evening shift had a significantly lower level of WHB than workers with other shifts. These differences are consistent with the theorization for building the Work-Health Balance questionnaire, in the sense that workers with a long-standing health problem will likely have more health needs, which in turn could make it more difficult to balance job demands (Gragnano et al., 2017). Lastly, work shifts showed a significant difference as expected, since the evidence of the relationship between health outcomes and this variable points to that direction (Jørgensen et al., 2017; Zhao et al., 2019). Here, we submit that WHB could contribute to a better understanding of how the managerial process and health needs can be related to shift work and its outcomes.
Thus, we believe that in Mexico the WHBq could be applied to develop workplace policies that seek to improve work environments to facilitate job retention and to achieve a better quality of life, preventing the developing of NCD's, as well as reducing work disabilities.
This study has several limitations. First, most of the sample consisted of administrative workers. Therefore, the sample of this study does not represent all kinds of workers. However, our sample grouped workers from various companies and occupation sectors, such as service, manufacture, health, and education, which are some of the main sectors in Mexico's economy (Observatorio Laboral, 2019).
Second, the results of concurrent and differential validity are only preliminary, and associations with other established variables in the literature, such as job demands or job stress, were not explored. However, the study provides strong evidence of the reliability of WHBq, and concurrent and differential validity was evaluated considering variables that are crucial within the WHB theory, such as the presence of a disease, age, and shift work (Tables 3 - 4).
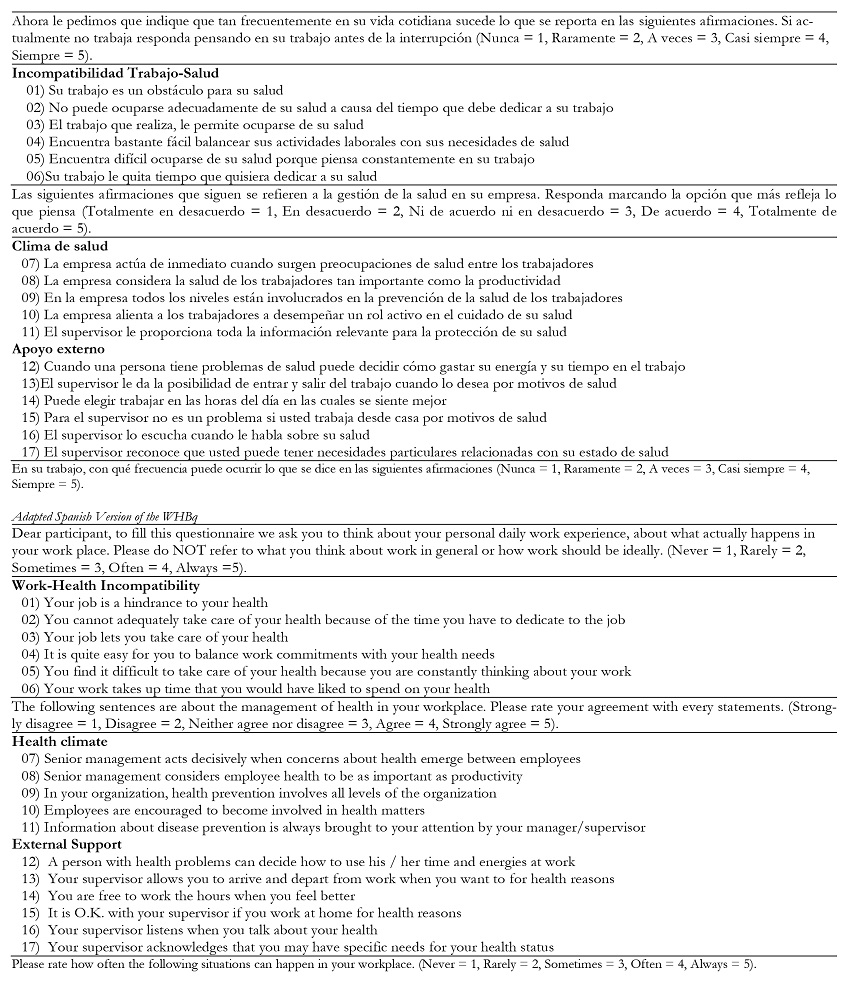
To a better understanding of the adapted Spanish version of the WHBq the adapted English version of the WHBq has been added to compare and contrast its content (Table 5).
Conclusion
The WHBq in its Spanish version shows good psychometric properties. There is still the need to analyze the convergent and predictive validity of this version of the questionnaire, comparing it with well-established variables, and studying possible relations to long-standing health problems. However, the translated questionnaire appears to be well comprehended by Mexican workers, and the model of the confirmatory factor analysis had a good fit. Therefore, this is a reliable and valid questionnaire for this population. Moreover, this is the first questionnaire that measures WHB available in Spanish, and we believe that in this country, it will prove to be a helpful and necessary instrument to achieve a better quality of life for workers in the future.

