










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkThe European Journal of Psychiatry
versión impresa ISSN 0213-6163
Eur. J. Psychiat. vol.28 no.3 Zaragoza jul./sep. 2014
https://dx.doi.org/10.4321/S0213-61632014000300004
Anxiety in patients with acute coronary syndromes
Snezana V. Ciric-Zdravkovic, MD, PhD*,**; Olivera V. Zikic, MD, PhD**,***; Dragana M. Stanojevic, MD, M.Sci* and Svetlana M. Petrovic-Nagorni, MD*
* Clinic for cardiovascular diseases, Clinical Center Nis, Serbia
** Medical Faculty University of Nis, Serbia
*** Clinic for Mental Health Protection, Clinical Center Nis, Serbia
ABSTRACT
Background and Objectives: Anxiety is frequently encountered in acute coronary syndrome. It is believed that the prevalence of anxiety among cardiac patients is between 15 and 50%. The goal of our study was to determine whether there is an association between current anxiety and anxiety tendency in patients with acute coronary syndrome. A secondary goal was to establish possible distinct features of acute coronary syndromes in patients with the anxiety.
Methods and results: Our study included 30 patients suffering from acute coronary syndrome. To obtain additional data on physical and mental health, we applied specially designed and validated questionnaires. In a groups without the anxiety and intensive anxiety there were no patients, while in the group with mild anxiety there were 21 patients (70%) and 9 patients had moderate anxiety (30%). The average number of hospital treatments was significantly higher in patients with moderate anxiety (average 2.3). Patients who were first time hospitalized due to cardiovascular disease, at the highest percentage (81%) had low current anxiety. Those patients who had intensive anxiety traits and propensity to anxiety response had the highest average number of hospital days (9 days). Patients who had intensive anxiety traits had the lowest values of internal locus of control (had feeling that only themselves were cause of the disease).
Conclusions: Current anxiety and anxious personality structure are strongly associated with the course of the coronary heart disease. In particular, this refers to the length of hospital stay and number of hospitalizations.
Key words: Acute coronary syndrome; Anxiety; Prognosis.
Introduction
It is a known fact that somatic disorders, in a certain percentage, are associated with a mental health problems, whether in a form of two co-existent diseases, whether psychological problems are only associated symptoms and/or response to somatic disease.
Anxiety is a psychological symptom frequently encountered in patients suffering from acute coronary syndrome. It is believed that the prevalence of anxiety among cardiac patients is between 15 and 50%. The prevalence of depression is also high in patients with coronary heart disease (CHD). Rates of major depressive disorder of near 15% have been found in patients with acute coronary disease. Recently, the EUROASPIRE III study on 8580 patients after hospitalization for coronary heart disease revealed that the proportion of patients with depression, measured by the Hospital Anxiety and Depression Scale, varied from 8.2 - 35.7% in men and 10.3 - 62.5% in women1,2.
In CHD patients undergoing elective percutaneous coronary interventions (PCI), lower anxiety levels are positively associated with survival and reduce the risk for major adverse coronary events (MACE) during the first five years after index PCI. The beneficial effects of anxiety on cardiovascular mortality and morbidity suggest that a differentiated approach to diagnosing and treating anxiety in CHD patients is warranted3.
In study with heart failure patients it was found that anxiety is a better prognostic indicator than depression and that anxiety increases the risk for 3-fold of unwanted cardiac events (myocardial infarction, sudden cardiac death)4. Anxiety is one of the established risk factors for sudden cardiac death. Several studies have demonstrated increased risk of sudden cardiac death in patients with phobic, generalized anxiety and panic disorders. Anxiety increases the mortality rate in patients with heart diseases by increasing the risk from ventricular arrhythmias and sudden cardiac death, consequently5. Continuation of exhibiting a high level of anxiety after the diagnosis of coronary artery disease is a significant risk factor for the development of myocardial infarction or death in these individuals6.
An increasing number of data from prospective studies show that negative emotions such as anxiety, anger and depression are risk factors for coronary artery disease. Several mechanisms explain this finding including links between negative emotions with bad habits such as smoking, nutritional habits, reduction of physical activity. Also emotional stress has the direct negative effect on the progression of atherosclerosis and it reduces threshold for ventricular arrhythmias and possibly sudden cardiac death7. Anxiety increases blood coagulability during and after the emotional stress, which is one of the mechanisms that may link this emotion and cardiac disease8. The possibility that anxiety and depressive symptoms and subsequent acute myocardial infarction are caused by subclinical manifestations of atherosclerosis is among the greatest challenges for researchers. Atherosclerosis may facilitate anxiety and depressive symptoms even before generating cardiac ischaemia creating a spurious circulus vitiosus. One possible pathway is the depressogenic actions of the increased inflammatory activity. Moreover, neuroimaging and neuropathology studies suggest that late onset depression often has a cerebrovascular origin. Cerebral atherosclerosis may thus facilitate depressive symptoms and anxiety even before coronary atherosclerosis generates cardiac ischaemia9.
Objective
Since previous studies found that anxiety is associated with CHD, the goal of our study was to determine whether there is an association between current anxiety and anxiety tendency in CHD patients. A secondary goal was to establish possible distinct features of acute coronary syndromes in patients with the anxiety. Specifically, we were interested in whether some variables in CHD are associated with current levels of anxiety or a general tendency towards anxiety reaction or specific type of personality.
Methods
Our study included 30 patients suffering from acute coronary syndrome (unstable angina pectoris, myocardial infarction with and without ST segment elevation - STEMI and NSTEMI) who were at the time of the study hospitalized at the Clinical Center of Nis. We included patients hospitalized at our Clinic for cardiovascular diseases during consecutive 7 days.
The study was performed according to the Good Clinical Practice guidelines and the Declaration of Helsinki. Study protocol was approved by the Ethic Committee of Clinical Centre Nis. Written informed consent was obtained from all participants prior to their inclusion in the study.
Patients were analyzed by standard procedures involving laboratory tests, ECG and echocardiography.
To obtain additional data, we applied the following questionnaires:
1. General questionnaire by which we obtained socio-demographic data and information on the progress of cardiac disease (duration of treatment, number of treatments), heredity, association with psychological stress disorders.
2. State and Trait Anxiety Inventory (STAI) - a questionnaire consisting of 40 questions to assess the intensity of the two forms of anxiety - the current level of anxiety (state of anxiety) and anxiety as a personality trait (trait anxiety). Based on the recently researches both types of anxiety can be divided into mild, moderate and intense anxiety. Also, by using the special table we transformed both primary scores into Z-scores (0-100) that allowed these two types of anxiety to be compared.
3. Health Locus of Control (LOC) - a questionnaire that measures where the patient places the center of disease control - internal (considers him/her to be dominantly responsible for their own health and the disease) and external (considers external factors such as chance or fate, doctors and other people to be crucial that he will get sick and/or be cured). By processing the result we got the intensity scores for:
(a) -Internal control center.
(b) -Control center linked to the coincidence/fate.
(c) -Control center linked to doctors.
(d) -Control center linked to the other persons.
After the division of the entire group of patients in the subgroups without anxiety and with mild, moderate and intensive anxiety, subgroups were mutually compared in relation to the clinical features of acute coronary syndrome (a type of disorder, localization of myocardial infarction, inflammatory markers, risk factors, laboratory findings, ECG findings, echocardiography results) and its progression.
Place of research
Research was conducted at the Clinic for cardiovascular diseases, Clinical Center Nis.
Statistical data
Data were analyzed in SPSS 12 program, continuous variables were correlated using T student test and ANOVA analysis, while chi-square test was used for categorical variables. We correlated numeric variables using Pearson's correlation.
Results
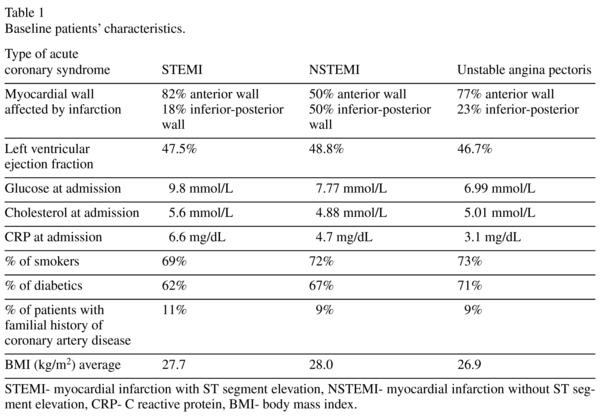
Study included 30 consecutive patients admitted to Coronary Care Unit during one week (19 males or 63.3% and 11 women or 36.7%), mean age 61.75 ± 8.4 years. We did not include comatose patients, those with severe hemodynamic and electromechanical complications of myocardial infarction, cerebrovascular insult (older or de novo) and massive hemorrhage due to aggressive antithrombotic therapy in this clinical setting. The baseline patients' characteristics are given in Table 1.
After patient division according to the levels of anxiety, in a groups without the anxiety and intensive anxiety there were no patients, while in the group with mild anxiety there were 21 patients (70%) and 9 patients had moderate anxiety (30%). In terms of anxiety traits - in a subgroup of patients with anxiety we found that 19 patients (63.33%) had mild, 9 patients had moderate (30%) and 1 patient had pronounced (6.67%) anxiety.
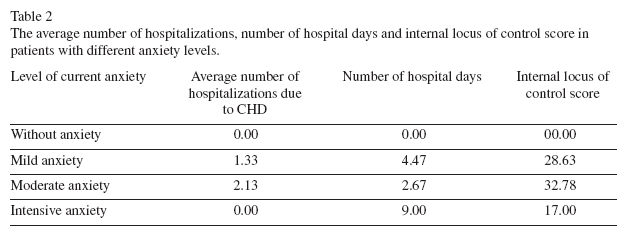
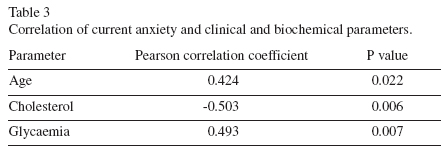
Statistical analysis showed a statistically significant relationship between several variables (Table 2). The average number of hospital treatments due to CHD was significantly higher in patients with moderate anxiety (average 2.3) than in those with mild anxiety (average 1.33) (F = 6.308, p = 0.018). Patients who were hospitalized first time due to cardiac causes had at the highest percentage (81%) low current anxiety, and with the increasing number of hospitalizations moderate anxiety was dominant (χ2 = 8.779, p = 0.012) (Figure 1). Those patients who had intensive anxiety traits and an inclination towards anxiety response had the highest average number of hospital days (9 days) (χ 2 = 25.427, p = 0.031). Patients who had intensive anxiety traits had the lowest values of internal locus of control (F = 5.379, p = 0.011). Current levels of anxiety positively correlated with the age and level of blood glucose, while they negatively correlated with cholesterol levels (Table 3). Anxiety traits positively correlated only with the number of hospitalizations due to CHD (r = 0.432, p = 0.019). Statistically significant negative correlation was found between internal locus of control and the number of patient days (r = -0.593, p = 0.001).

Discussion
Data obtained in this study indicate that anxiety has a much greater influence on the course of coronary artery disease than its clinical correlates. It has been shown that patients who have two or more hospitalizations due to coronary heart disease with new hospitalization have higher levels of anxiety. This information is important given that the literature has repeatedly emphasized the negative impact of anxiety on the outcome of coronary artery disease and it is considered that anxiety actually worsens the outcome of the disease6. Based on these data and data from the literature we can say that patients with a higher number of hospitalizations due to higher intensity of current anxiety are at a higher risk of re-infarction and lethal outcome.
Also those people, who basically were very anxious, had a significantly higher number of hospital days spent in a coronary care unit. Since the longer hospitalizations are associated with resistant symptoms or complications, patients with high basic anxiety probably have a tendency toward more severe disease and additional complications, which can only be confirmed by the new study specifically structured. Interestingly, patients who were extremely anxious basically have the lowest level of internal locus of control, which means that they think they have very low influence on the course and outcome of disease. This fact can de-motivate the patient to change behavior to that which will help to reduce the number of risk factors and reduce the likelihood of new coronary events. Also, an internal locus of control negatively correlated with the number of hospital days, which means that those patients who have the impression that both they and medical professionals influence the outcome of the disease have a shorter hospital stay.
Current anxiety positively correlated with the age and blood glucose levels. This means that we can expect that elderly have a higher intensity of anxiety and consequently a higher risk for adverse outcome. Similarity exists with the level of blood glucose level, which is a significant risk factor for coronary heart disease and its complications.
It is interesting that anxiety negatively correlated with the level of cholesterol. This means that people with high levels of anxiety have lower cholesterol. In studies it is typically found that the anxiety is associated with higher levels of serum cholesterol while the depression and suicidal tendencies are associated with reduced levels of cholesterol. In the literature we found conflicting evidence of a relationship between statins and mood. Further research is recommended in particular with older, female and lower socioeconomic status samples10,11.
Anxious traits in correlative analysis were clearly related with the number of hospital treatments which means that for patients with CHD who have a high basic anxiety we can expect a greater number of health deteriorations or acute coronary syndromes.
Conclusion
Current anxiety and anxious personality structure are strongly associated with the course of the coronary heart disease. In particular, this refers to the length of hospital stay and number of hospitalizations.
References
1. Herrmann-Lingen C. Anxiety and depression in cardiology patients: how to diagnose, how to treat? Herz. 2001; 26 (5): 326-334. [ Links ]
2. Colquhoun DM, Bunker SJ, Clarke DM et al. Screening, referral and treatment for depression in patients with coronary heart disease a consensus statement from the National Heart Foundation of Australia. Med J Aust. 2013; 198 (9): 483-484. [ Links ]
3. Meyer T, Hussein S, Lange HW, Herrmann-Lingen C. Anxiety is associated with a reduction in both mortality and major adverse cardiovascular events five years after coronary stenting. Eur J Prev Cardiol. 2014 (Epub ahead of print). [ Links ]
4. Strik JJMH, Denollet J, Lousberg R, Honig A.Comparing symptoms of depression and anxiety as predictors of cardiac events and increased health care consumption after myocardial infarction. J Am Coll Cardiol. 2003; 42: 1801-1807. [ Links ]
5. Kawachi I, Sparrow D, Vokonas PS, Weiss ST. Symptoms of anxiety and risk of coronary heart disease: The Normative Aging Study. Circulation. 1994; 90: 2225-2229. [ Links ]
6. Shibeshi WA, Young-Xu Y, Blatt CM. Anxiety Worsens Prognosis in Patients With Coronary Artery Disease. J Am Coll Cardiol. 2007; 49: 2021-2027. [ Links ]
7. Denollet J, Pedersen SS. Anger, Depression, and Anxiety in Cardiac Patients: The Complexity of Individual Differences in Psychological Risk. J Am Coll Cardiol. 2009; 53: 947-949. [ Links ]
8. von Känel R, Dimsdale JE, Adler KA, Patterson TL, Mills PJ, Grant I. Effects of depressive symptoms and anxiety on hemostatic responses to acute mental stress and recovery in the elderly. Psych Res. 2004; 126: 253-264. [ Links ]
9. Gustad LT, Laugsand LE, Janszky I, Dalen H, Bjerkeset O. Symptoms of anxiety and depression and risk of acute myocardial infarction: the HUNT 2 study. Eur Heart J. 2014; 35 (21): 1394-1403. [ Links ]
10. Papakostas GI, Öngür D, Iosifescu DV, Mischoulon D, Fava M. Cholesterol in mood and anxiety disorders: review of the literature and new hypotheses. European Neuropsychopharmacology. 2004; 14 (2): 135-142. [ Links ]
11. While A, Keen L. The effects of statins on mood: a review of the literature. Eur J Cardiovasc Nurs. 2012; 11: 85-96. [ Links ]
![]() Correspondence:
Correspondence:
Dr. Dragana Stanojevic
Clinic for cardiovascular diseases
Clinical Center Nis
Bulevar dr Zorana Djindjica 48
18000 Nis Serbia
Phone: +381643068447
Fax: +381184221674
E-mail draganastanojevic1@gmail.com
Received: 22 January 2014
Revised: 5 April 2014
Accepted: 13 June 2014

