










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkThe European Journal of Psychiatry
Print version ISSN 0213-6163
Eur. J. Psychiat. vol.29 n.2 Zaragoza Apr./Jun. 2015
https://dx.doi.org/10.4321/S0213-61632015000200004
An abbreviated version of the brief assessment of cognition in schizophrenia (BACS)
Yasuhiro Kaneda, MD, PhDa and Richard S.E. Keefe, PhDb
a Department of Psychiatry, Iwaki Clinic, Anan, Tokushima 774-0014, Japan
b Department of Psychiatry and Behavioral Sciences, Duke University Medical Center, Durham, NC 27710, USA
ABSTRACT
Background and Objectives: A short version of the Brief Assessment of Cognition in Schizophrenia (BACS) was derived.
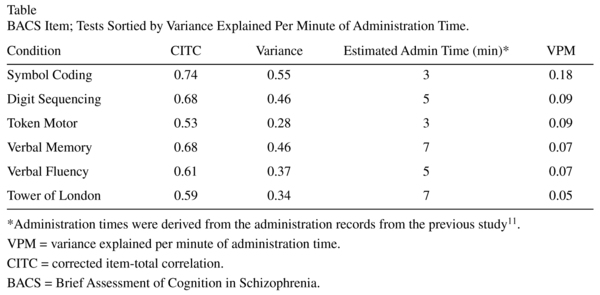
Methods: We calculated the corrected item-total correlation (CITC) for each test score relative to the composite score, and then computed the proportion of variance that each test shares with the global score excluding that test (Rt2 = CITCt2) and the variance explained per minute of administration time for each test (Rt2/mint).
Results and Conclusions: The 3 tests with the highest Rt2/mint, Symbol Coding, Digit Sequencing, and Token Motor, were selected for the Abbreviated BACS.
Key words: Schizophrenia; Cognition; Clinical assessment.
Introduction
The assessment of cognitive function is an important step in evaluating patients with schizophrenia because of the extensive evidence that cognitive impairment is a core feature of schizophrenia1, as well as a key determinant of functional outcome2. The Brief Assessment of Cognition in Schizophrenia (BACS) has been developed as a quick and efficient tool for measuring cognition in patients with schizophrenia3. The time required for the testing with the BACS is approximately 30 min with minimal extra time for scoring and training demands. The author tried to derive an abbreviated version of the BACS (Abbreviated BACS, A-BACS) to make it more useful for clinical work, using the Japanese BACS recently developed by the authors upon permission4.
Methods
Data from a previous study were utilized, and the subjects consisted of 472 stable patients with a DSM-IV5 diagnosis of chronic schizophrenia or schizoaffective disorder. Among the patients, 213 (45%) were women; the patients had a mean age of 38.8 (SD = 13.3), and a mean age at onset of 24.7 years (SD = 7.9).
The BACS takes approximately 30 min, and is devised for easy administration and scoring by non-psychologists. It is specifically designed to measure treatment-related improvements. The BACS has high test-retest reliability3, and is as sensitive to cognitive dysfunction in schizophrenia as standard 2.5-h batteries6. The BACS includes brief assessments of verbal memory (Verbal Memory), working memory (Digit Sequencing), motor speed (Token Motor), verbal fluency (Verbal Fluency), attention and processing speed (Symbol Coding), and executive function (Tower of London). The 18-item Brief Psychiatric Rating Scale (BPRS7, 1-7 score) was completed by a trained psychiatrist along with the BACS, and the patients had a mean total BPRS score of 42.0 (SD = 13.6).
The data analyses were conducted using JMP-8.0.2.J for Mac software (SAS Institute Inc., Cary, NC, US). Descriptive statistics were used to report the patients in terms of socio-demographic and clinical data. The relationships among measures were determined by calculating Pearson correlations (r) among the scores. The level of significance was set at P < 0.05 (two-tailed).
Results
Based on the previous study8, we calculated the corrected item-total correlation (CITC) for each test score relative to the composite score (Table). The CITC is the correlation between each standardized test score in the BACS with the standardized BACS total score excluding the test score itself, thereby controlling for part-whole correlation. We computed the proportion of variance that each test shares with the global score excluding that test (Rt2 = CITCt2) and the variance explained per minute of administration time for each test (Rt2/mint). The 3 tests with the highest Rt2/mint were selected for the A-BACS. The composite score from the Symbol Coding, Digit Sequencing, and Token Motor tasks correlated 0.93 with the composite score of the whole BACS (R2 = 0.86, P < 0.0001) and correlated 0.74 with the total battery score excluding these 3 tests (R2 = 0.55, P < 0.0001).
Discussion
The A-BACS is also composed of two speed of processing measures and one working memory measure. The finding is consistent with the results in the previous reports: in their report, Hurford et al.8 proposed a group of tests composed of trail making B, category fluency, and digit symbol. Verbal fluency was not chosen for this A-BACS, mainly because verbal fluency in the BACS is composed of Semantic Fluency and two trials of Letter Fluency, and thus it takes three times as long as Semantic Fluency alone takes. The findings in this study therefore suggested that the A-BACS could provide a valid estimate of general cognitive ability.
For assessing cognitive function in schizophrenia, a neuropsychological test battery (NTB), usually consisting of 8-12 tests tapping each of several for the putative neurocognitive domains, is employed. These NTBs are, however, time consuming, technically difficult, and costly. The availability of a quick and efficient tool for measuring cognition in patients with schizophrenia could be an extremely useful guide for clinicians making decisions about potential rehabilitation, and thus BACS has been developed. Still, a typical outpatient psychiatric practice allots about 15min for medication management appointments8. The 3 tests with the highest Rt2/mint were selected for the A-BACS, because, as Hurford et al.8 described, a brief battery should be very brief and account for a large proportion of the variance of the global cognitive score of the battery.
Since a single generalized cognitive deficit has been suggested to best characterizes schizophrenia9 and A-BACS could be administered approximately in 11 min, it may be a good choice to use an A-BACS to assess cognitive function in patients with schizophrenia in clinical settings. For broader dissemination of brief neuropsychological assessments such as A-BACS, further studies should be necessary to test their sensitivity to treatments. In addition, we should be aware that, for prediction of different aspects of outcome, another A-BACS composed of a different subset may be necessary10.
Conflict of interest
Dr. Kaneda is responsible for developing the Japanese version of the BACS. Dr. Keefe receives royalties from the BACS testing battery and the MATRICS Battery (BACS Symbol Coding). He is also a shareholder in NeuroCog Trials, Durham, NC, USA.
References
1. Mohamed S, Paulsen JS, O'Leary D, Arndt S, Andreasen N. Generalized cognitive deficits in schizophrenia: A study of first-episode patients. Arch Gen Psychiatry. 1999; 56(8): 749-54. [ Links ]
2. Green MF, Kern RS, Braff DL, Mintz J. Neurocognitive deficits and functional outcome in schizophrenia: Are we measuring the "right stuff"? Schizophr Bull. 2000; 26(1): 119-36. [ Links ]
3. Keefe RS, Goldberg TE, Harvey PD, Gold JM, Poe MP, Coughenour L. The Brief Assessment of Cognition in Schizophrenia: Reliability, sensitivity, and comparison with a standard neurocognitive battery. Schizophr Res. 2004; 68(2-3): 283-97. [ Links ]
4. Kaneda Y, Sumiyoshi T, Keefe R, Ishimoto Y, Numata S, Ohmori T. Brief assessment of cognition in schizophrenia: Validation of the Japanese version. Psychiatry Clin Neurosci. 2007; 61(6): 602-9. [ Links ]
5. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV). Washington, D.C.: American Psychiatric Association. 1994. [ Links ]
6. Hill SK, Sweeney JA, Hamer RM, Keefe RS, Perkins DO, Gu H, et al. Efficiency of the CATIE and BACS neuropsychological batteries in assessing cognitive effects of antipsychotic treatments in schizophrenia. J Int Neuropsychol Soc. 2008; 14(2): 209-21. [ Links ]
7. Overall JE, Gorham DR. The brief psychiatric rating scale. Psychol Rep. 1962; 10: 799-812. [ Links ]
8. Hurford IM, Marder SR, Keefe RS, Reise SP, Bilder RM. A brief cognitive assessment tool for schizophrenia: Construction of a tool for clinicians. Schizophr Bull. 2011; 37(3): 538-45. [ Links ]
9. Bilder RM, Goldman RS, Robinson D, Reiter G, Bell L, Bates JA, et al. Neuropsychology of first-episode schizophrenia: Initial characterization and clinical correlates. Am J Psychiatry. 2000; 157(4): 549-59. [ Links ]
10. Harvey PD, Keefe RS, Patterson TL, Heaton RK, Bowie CR. Abbreviated neuropsychological assessment in schizophrenia: Prediction of different aspects of outcome. J Clin Exp Neuropsychol. 2009; 31(4): 462-71. [ Links ]
11. Keefe RS, Harvey PD, Goldberg TE, Gold JM, Walker TM, Kennel C, et al. Norms and standardization of the Brief Assessment of Cognition in Schizophrenia (BACS). Schizophr Res. 2008; 102(1-3): 108-15. [ Links ]
![]() Correspondence:
Correspondence:
Yasuhiro Kaneda, MD, PhD
Department of Psychiatry
Iwaki Clinic, 11-1 Kamimizuta
Gakubara, Anan
Tokushima 774-0014
Japan
Tel. +81-884-23-5600
Facsimile number: +81-884-22-1780
E-mail: kaneday-tsh@umin.ac.jp
Received: 24 December 2014
Revised: 31 March 2015
Accepted: 31 March 2015

