










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkThe European Journal of Psychiatry
versión impresa ISSN 0213-6163
Eur. J. Psychiat. vol.30 no.4 Zaragoza oct./dic. 2016
Comparisons of verbal fluency brain correlates between adults and adolescents suffering from schizophrenia spectrum disorders: A pilot study
Sébastien Urbena,1; Laure Jaugeya,1; Eleonora Fornarib; Pierre Magistrettic,d; Pierre Marqueta,c, Laurent Holzera and Pascal Vianina,1
a Departement of Psychitary, University Hospital of Lausanne (CHUV), Lausanne. Switzerland
b Biomedical Imaging Center (CIBM), Department of Radiology, CHUV. Switzerland
c Center for Psychiatric Neurosciences (CPN), Lausanne. Switzerland
d Brain Mind Institute, EPFL, Lausanne. Switzerland
ABSTRACT
Background and Objectives: Prefrontal cortex (PFC) dysfunctions leading to cognitive deficits refer to a core feature of schizophrenia spectrum disorders (SSD). This exploratory study compares the effect of SSD on two stages of maturation of PFC.
Methods: Using functional magnetic resonance imaging (fMRI), we measured the brain correlates related to a verbal fluency task (a hallmark executive function test) in 12 patients with SSD: 6 adolescents (SSD-ado) and 6 adults (SSD-adu).
Results SSD-ado showed greater activation in insula, thalamus and hIP1 whereas SSD-adu recruited more intensively precentral gyrus and temporal pole to resolve the task. Thus, adolescents with SSD seem to adopt less frontal mediated strategic processes. In contrast, adults seem to be able to use PFC mediated strategy despite the well-known deleterious effect of SSD on the PFC.
Conclusions This first exploratory study revealed that adults and adolescents with SSD seemed not to use the same strategy to resolve a verbal fluency task. Thus, despite the illness, which is known to have a deleterious influence on PFC, adult patients seem to be able to recruit these resources to perform an executive function task. Further studies are needed in order to confirm and extend these new and preliminary results.
Keywords: Schizophrenia spectrum disorders; Executive functions; Prefrontal cortex; Brain maturation; Adolescence; Adulthood.
Significant outcomes
Adolescents with schizophrenia spectrum disorders used verbally mediated strategies to resolve a verbal fluency task.
Adults with schizophrenia spectrum disorders used frontal mediated strategies to resolve a verbal fluency task.
This is the first study exploring the effects of schizophrenia spectrum disorders on brain correlates of executive functions in two different stages of maturation of the prefrontal cortex.
Limitations
Small sample size which hampered a wide generalization of the results.
Absence of control groups which prevent from comparison with the typical development of verbal networks.
Introduction
Schizophrenia spectrum disorders (SSD) encompass a wide range of disorders such as schizophrenia and psychosis. Thus, SSD refers to severe mental disorders emerging from complex and multifactorial etiology, with a prevalence rate of 4.6/1000 people1. The core symptoms might broadly be categorized in (a) positive symptoms (e.g., hallucinations), (b) negative symptoms (e.g., social withdrawal), (c) affective symptoms (e.g., flattened affect), and (d) cognitive symptoms (e.g., executive function deficits)2. The first signs of SSD generally occur during adolescence3. In many cases, SSD refers to severe disabilitating disease with frequent relapse and chronic time-course.
More specifically, cognitive symptoms in SSD lead to impairments in everyday life and drastically reduce quality of life4. Cognitive deficits have been thought to be primary and core dysfunctions in SSD5,6. Indeed, cognitive deficits affect up to 80% of patients with SSD and are associated with frontal lobe abnormalities7. Furthermore, cognitive dysfunctions are stable and persist throughout the course of the illness, and are even present during remission phases5. More specifically, in adolescents with SSD, cognitive disabilities were found to be even more severe than in adults and to contribute to less independence, poorer school achievement, vocational failure and social relationships problems in adult life8,9.
In particular, numerous studies demonstrated an alteration of frontal lobe in SSD10,11. More specifically, patients with SSD were reported to present word generation alteration or initiation skills deficits12. Such deficits are present early in the time-course of SSD13 and lead to severe impairments in everyday life4,14. Such abilities could be well measured with the verbal fluency task, an executive task within the most sensitive to assess frontal lobe deficits15.
In particular, prefrontal cortex (PFC) functioning which sustained word generation and initiation skills, were assessed in adults with SSD. Indeed, functional Magnetic Resonance Imaging (fMRI) studies demonstrated that adults with SSD, compared to healthy participants, showed reduced recruitment of the inferior prefrontal regions, the anterior cingulate and the middle frontal cortices in order to resolve a verbal fluency task (see meta-analysis16). Nevertheless, to the best of our knowledge, no study explored the brain correlates underlying verbal fluency in adolescents with SSD, despite the fact that the PFC has a protracted maturation until young adulthood, up to 20 years17.
Aims of the study
In this perspective, the current study aimed to examine the impact of SSD on PFC in two different stage of maturation of the PFC, namely when fully developed (young adulthood) or in development (adolescence). Such a study was never undertaken before and it could give important information about the moderation impact of development of SSD on PFC. Therefore, the present exploratory pilot study examined using fMRI, the brain correlates sustaining verbal fluency performance (i.e., executive function) which was measured in 6 young adults with SSD and in 6 adolescents with SSD (comparable in terms of duration of illness, DOI).
Material and methods
Participants
All patients were(1) right-handed; (2) fulfilled the criteria for schizophrenia or psychotic disorders (e.g., schizophrenia, psychotic disorders NOS, schizophreniform disorders, schizoaffective disorders) according to the Diagnostic and Statistical Manual, 4th ed. and (3) received atypical antipsychotic medication. Patients with histories of traumatic brain injury, epilepsy, alcohol and substance abuse, or other diagnosed neurological conditions were excluded from the study. All patients were clinically stabilized (i.e., stable medication, no recent relapse, stable way of life). Participants provided informed written consent and the protocol was approved by the ethical committee of the medical faculty of Lausanne University.
The 12 patients with SSD enrolled in the study were split into two groups (matched for gender and DOI) (1) 6 young adults patients (SSD-adu) and (2) 6 adolescents (SSD-ado).
Measures
Clinical measures
The clinical status of patients were assessed with the Positive and Negative Symptom Scale18. This scale is composed of three subscales: positive symptoms (seven items), negative symptoms (seven items), and general psychopathology (sixteen items). The two groups did not show any significant differences on the three subscales. Table 1 summarizes the socio-demographic as well as the clinical measures of the sample.

Covert verbal fluency task
The verbal fluency task19 was given within an fMRI block design, with an alternation of four active and four rest blocks. Each of the 8 blocks lasted 25 seconds. During the active condition, participants were instructed to silently (in order to avoid excessive motions, see20) produce as many words as possible beginning with a letter (i.e., P, A, T, M) visually presented during the 25 seconds period (one letter per active block). After the task, a debriefing was done with the participants to ensure that they realize the task. During the rest condition, patients saw a black screen and were instructed to relax. Each block consisted of 5 volumes. Presentation of stimuli was controlled by the E-Prime software package (Psychology Software Tools, Pittsburg, USA).
Magnetic resonance imaging
Image acquisition and processing
Participants underwent a MRI session in a 3T-Trio scanner (Siemens Medical System). The protocol included a high resolution T1 weighted acquisition and an fMRI session performed with a single-shot echo-planar gradient-echo-pulse sequence (EPI, TR = 5000 ms, TE = 30 ms, flip angle = 90o, field of view = 256 mm). The acquired volume included 28 axial slices (matrix size 128*128 with 4 mm slice thickness), was aligned with the anterior-posterior commissure line and covered the whole brain. Images were preprocessed with SPM5 (http://www.fil.ion.ucl.ac.uk/spm/).
Functional images were corrected for motions by rigid body transformation that optimized the realignment of each volume with the first of the session. Notice that the estimated movement parameters were then included as nuisance variables in statistics at single subject-level, in order to exclude possible residual spurious activation due to head movement beyond the correction done by realignment. Then, functional images were coregistered with the high resolution T1-weighted acquisition. The anatomical images were normalized to the MNI T1 template by affine transformation and the estimated normalization parameters were applied to the functional images, which were finally smoothed with an 8-mm Gaussian kernel in order to increase signal-to-noise ratio.
Data analyses
Statistical analyses were performed for each subject according to the General Linear Model and contrasts of interest were computed for each individual (activity condition versus rest condition). Then, contrasts of interest (i.e. β estimates for the specified contrasts) were sort as basis for group results based on random effect analyses. First, the networks recruited when completing the fluency task was assessed for each group separately (SSD-adu and SSD-ado) by means of one-sample T-tests. These analyses were performed in order to (1) observe the networks recruited in SSD-ado as it was never tested before and (2) assure that the patients performed the fluency task. Second, in order to assess group differences, the same contrasts (verbal fluency versus rest) were compared between groups, by computing two sample t-tests. In accordance to the exploratory nature of this pilot study, the statistical maps were thresholded at a level of significance of puncorrected <.001 and cluster size (k) > 10 contiguous voxels.
Results
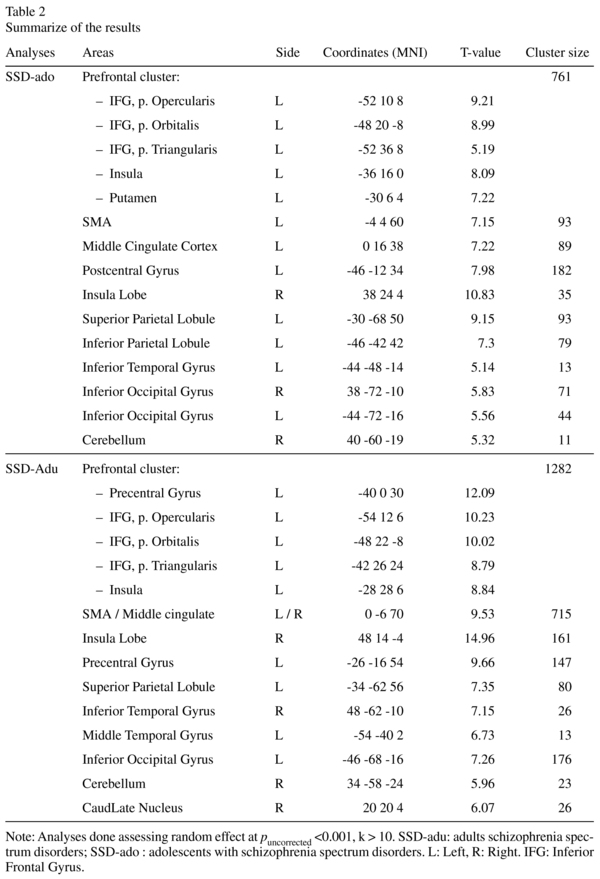
The two groups recruited a comparable wide network mainly located in frontal, parietal and temporal regions (see Table 2 for details).
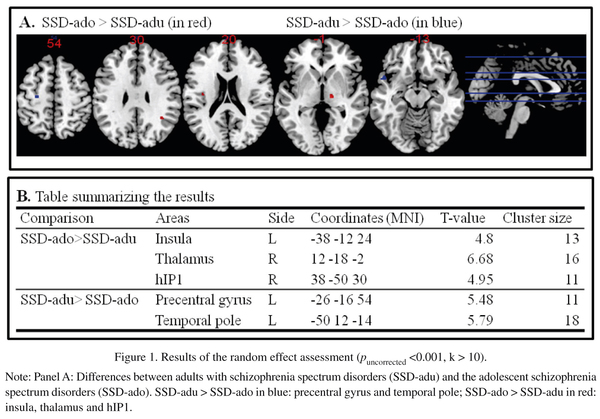
The SSD-adu when contrasted to SSD-ado recruited more intensively the precentral gyrus and the temporal pole to resolve the fluency task. The SSD-ado when contrasted to the SSD-adu showed greater activation in the insula, the thalamus and the hIP1 (see Figure 1).
Discussion
We explored, in patients with SSD, the brain activity related to a hallmark test of PFC functions (i.e., verbal fluency task) in two different stages of maturation of the PFC.
First, consistently with previous studies21, the verbal fluency task recruits a wide fronto-parieto-temporal networks to be solved. These networks are analogous for adolescents and adults suffering from SSD. It is noteworthy that it is the first time that a study explored the brain activity related to verbal fluency in a sample of adolescents with SSD.
Second, results indicated that adolescents with SSD recruited more intensively the insula and the thalamus which were related to language and memory processes. More specifically, the thalamus was reported to maintain verbal information in memory process22 and the left insula to prearticulatory function and programming vocal gestures23. In addition, the hIP1 was shown to be strongly linked to the left insula24 and related to semantic knowledge25. Taken together these results with the fact the PFC showed a protracted maturation until adulthood17, we might hypothesize that in order to perform the fluency task, adolescents with SSD adopted strategy mediated by semantic and language processes in contrast to strategies mediated by executive functions which are sustained by PFC.
However, adults with SSD compared to adolescents with SSD activated more intensively the precentral area which was reported to be involved in the verbal fluency performance26 and the temporal pole which was related to executive function deficits at early stage of dementia27. Thus, despite the illness, which is known to have a deleterious influence on PFC28, adult patients seem to be able to recruit these resources to perform an executive function task. These preliminary findings suggest a possible recruitment of frontal areas despite the course of the illness at least, when the PFC was fully developed before the apparition of the pathology. In this perspective, further studies including healthy control participants and longitudinal design are warranted in order to better understand the evolution of the PFC underlying the performance in such a type of task within SSD time-course.
Some limitations of the present study may be stressed. This study had an exploratory purpose regarding the lack of data in the literature. In this perspective, the study was conducted on a small sample which may get the generalization of the results difficult. An intra-subject longitudinal design may have been a better design rather than this cross-sectional design introducing between-subjects variability. Furthermore, the use of covert verbal fluency task did not allow the evaluation of the performances. Thus, we were not able to highlight the possible link between the brain activity and behavioral aspects. An additional aspect, that should be explored in further studies, is the comparison between the typical development of verbal networks and the possible alteration induced by SSD.
Despites its limitations, this pilot study opened new perspectives in the examination of PFC development during the SSD time course. Indeed, it is, to the best of our knowledge, the first study which explored the effects of SSD on brain correlates of verbal fluency in two different stages of maturation of the PFC. The intriguing results found in the current study are to be further explored.
Acknowledgment
The authors wish to express their gratitude to the participants for agreeing to participate in the study.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Statement of interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
1 Sébastien Urben and Laure Jaugey contributed equally as first author to the paper.
References
1. Saha S, Chant D, Welham J, McGrath J. A systematic review of the prevalence of schizophrenia. PLoS medicine. 2005; 2(5): e141. [ Links ]
2. Kar SK, Jain M. Current understandings about cognition and the neurobiological correlates in schizophrenia. Journal of neurosciences in rural practice. 2016; 7(3): 412-8. [ Links ]
3. Sham PC, MacLean CJ, Kendler KS. A typological model of schizophrenia based on age at onset, sex and familial morbidity. Acta psychiatrica Scandinavica. 1994; 89(2): 135-41. [ Links ]
4. Stip E. Cognition, schizophrenia and the effect of antispychotics. Encephale. 2006; 32: 341-50. [ Links ]
5. Gold JM. Cognitive deficits as treatment targets in schizophrenia. Schizophrenia research. 2004; 72(1): 21-8. [ Links ]
6. Nuechterlein KH, Ventura J, Subotnik KL, Bartzokis G. The early longitudinal course of cognitive deficits in schizophrenia. The Journal of clinical psychiatry. 2014; 75 Suppl 2: 25-9. [ Links ]
7. Medalia A, Choi J. Cognitive remediation in schizophrenia. Neuropsychology review. 2009; 19(3): 353-64. [ Links ]
8. Bark N, Revheim N, Huq F, Khalderov V, Ganz ZW, Medalia A. The impact of cognitive remediation on psychiatric symptoms of schizophrenia. Schizophr Res. 2003; 63(3): 229-35. [ Links ]
9. Wykes T, Newton E, Landau S, Rice C, Thompson N, Frangou S. Cognitive remediation therapy (CRT) for young early onset patients with schizophrenia: an exploratory randomized controlled trial. Schizophr Res. 2007; 94(1-3): 221-30. [ Links ]
10. Barch DM, Ceaser A. Cognition in schizophrenia: core psychological and neural mechanisms. Trends in cognitive sciences. 2012; 16(1): 27-34. [ Links ]
11. Senkowski D, Gallinat J. Dysfunctional Prefrontal Gamma-Band Oscillations Reflect Working Memory and Other Cognitive Deficits in Schizophrenia. Biological psychiatry. 2015. [ Links ]
12. Green MF, Kern RS, Heaton RK. Longitudinal studies of cognition and functional outcome in schizophrenia: implications for MATRICS. Schizophrenia research. 2004; 72(1): 41-51. [ Links ]
13. Goldberg TE, Aloia MS, Gourovitch ML, Missar D, Pickar D, Weinberger DR. Cognitive substrates of thought disorder, I: the semantic system. Am J Psychiatry. 1998; 155(12): 1671-6. [ Links ]
14. Green MF. What are the functional consequences of neurocognitive deficits in schizophrenia? The American Journal of Psychiatry. 1996; 153(3): 321-30. [ Links ]
15. Ikezawa K, Iwase M, Ishii R, Azechi M, Canuet L, Ohi K, et al. Impaired regional hemodynamic response in schizophrenia during multiple prefrontal activation tasks: A two-channel near-infrared spectroscopy study. Schizophrenia research. 2009; 108(1-3): 93-103. [ Links ]
16. Minzenberg MJ, Laird AR, Thelen S, Carter CS, Glahn DC. Meta-analysis of 41 functional neuroimaging studies of executive function in schizophrenia. Arch Gen Psychiatry. 2009; 66(8): 811-22. [ Links ]
17. Diamond A. Normal development of prefrontal cortex from birth to young adulthood: Cognitive functions, anatomy, and biochemistry. In: Stuss DT, Knight RT, editors. Principles of Frontal Lobe's Function. New York: Oxford University Press; 2002. p. 466-503. [ Links ]
18. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987; 13(2): 261-76. [ Links ]
19. Benton AL. Differential behavioural effects in frontal lobe disease. Neuropsychologia. 1968; 6(53-60). [ Links ]
20. Bullmore ET, Brammer MJ, Rabe-Hesketh S, Curtis VA, Morris RG, Williams SC, et al. Methods for diagnosis and treatment of stimulus-correlated motion in generic brain activation studies using fMRI. Human brain mapping. 1999; 7(1): 38-48. [ Links ]
21. Frith CD, Friston KJ, Herold S, Silbersweig D, Fletcher P, Cahill C, et al. Regional brain activity in chronic schizophrenic patients during the performance of a verbal fluency task. The British journal of psychiatry : the journal of mental science. 1995; 167(3): 343-9. [ Links ]
22. Moore AB, Li Z, Tyner CE, Hu X, Crosson B. Bilateral basal ganglia activity in verbal working memory. Brain and language. 2012. [ Links ]
23. Ackermann H, Riecker A. The contribution of the insula to motor aspects of speech production: a review and a hypothesis. Brain and language. 2004; 89(2): 320-8. [ Links ]
24. Uddin LQ, Supekar K, Amin H, Rykhlevskaia E, Nguyen DA, Greicius MD, et al. Dissociable connectivity within human angular gyrus and intraparietal sulcus: evidence from functional and structural connectivity. Cerebral cortex. 2010; 20(11): 2636-46. [ Links ]
25. Binder JR, Desai RH, Graves WW, Conant LL. Where is the semantic system? A critical review and meta-analysis of 120 functional neuroimaging studies. Cerebral cortex. 2009; 19(12): 2767-96. [ Links ]
26. McGraw P, Mathews VP, Wang Y, Phillips MD. Approach to functional magnetic resonance imaging of language based on models of language organization. Neuroimaging clinics of North America. 2001; 11(2): 343-53. [ Links ]
27. Schroeter ML, Vogt B, Frisch S, Becker G, Barthel H, Mueller K, et al. Executive deficits are related to the inferior frontal junction in early dementia. Brain : a journal of neurology. 2012; 135(Pt 1): 201-15. [ Links ]
28. Tomelleri L, Jogia J, Perlini C, Bellani M, Ferro A, Rambaldelli G, et al. Brain structural changes associated with chronicity and antipsychotic treatment in schizophrenia. European neuropsychopharmacology : the journal of the European College of Neuropsychopharmacology. 2009; 19(12): 835-40. [ Links ]
![]() Correspondence:
Correspondence:
Sébastien Urben
Research Unit, University Service of Child and
Adolescent Psychiatry
Av. Echallens 9, 1004 Lausanne, Suisse
Phone: +41 21 314 74 92
Fax: +41 21 314 74 81
E-mail: Sebastien.Urben@chuv.ch
Received: 19 January 2016
Revised: 27 July 2016
Accepted: 4 August 2016
