










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.97 no.2 Madrid feb. 2005
| POINT OF VIEW |
Tridimensional (3D) ultrasonography
F. Muñoz Agel and M. J. Varas Lorenzo
Unit of Echoendoscopy. Centro Médico Teknon. Barcelona, Spain
ABSTRACT
A review and update on tridimensional ultrasonography covering all its aspects, ultrasonography and 3D endoscopic ultrasonography, its technical details and current indications, such as volume calculation, vascular architecture assessment, and role in interventionist ultrasounds.
Images included are from the author's own experience.
Key words: Echography. Three-dimensional (3D) ultrasonography. 3D endoscopic ultrasonography. 3D endorectal ultrasonography. 3D laparoscopic ultrasonography.
Muñoz Agel F, Varas Lorenzo MJ. Tridimensional (3D) ultrasonography. Rev Esp Enferm Dig 2005; 97: 125-134.
Recibido: 16-02-04.
Aceptado: 11-05-04.
Correspondencia: M. J. Varas Lorenzo. Unidad de Ecoendoscopia. Centro Médico Teknon. C/ Marquesa de Vilallonga 12. 08017 Barcelona. Tel.: 932 906 434. Fax: 934 172 302.
e-mail: varas@dr.teknon.es
INTRODUCTION AND TECHNICAL OVERVIEW
The importance of three-dimensional imaging -currently including computerized tomography (CT) and magnetic resonance imaging (MRI) techniques- is unanimously accepted, since not only the exact location of a given lesion, but also its relations to neighboring structures and organs may be accurately studied; most importantly, a lesion's continuity may be assessed, particularly in infiltrating neoplastic growths. It also allows an accurate measurement of volume in expanding lesions and hence therapy planning, which is particularly relevant for liver tumors undergoing alcoholization, injection of antitumor agents, or therapy with radiofrequency waves, shock waves, etc., as well as response monitoring.
To obtain these three-dimensional images, all scanned data for a given volume are classified by a specific software program to allow spatial reconstruction. Acquiring images via CT or MRI is relatively straightforward, since the scanning system in both modalities is automatic, and the various slices for a selected region are sequentially obtained, which represents no major challenge for the explorer. Difficulties may only arise from organ displacement during breathing in some patients unable to cooperate, as subjects should stay frozen during scans.
However, the three-dimensional reconstruction of images may be rather more complex for ultrasonography, since the various 2D slices are manually obtained -rather than automated- using conventional ultrasound, and hence image acquisition depends on the explorer's skills. In addition, the number of slices that may be obtained is incalculable with no established start or end, since one more slice is always feasible. Despite these drawbacks, various systems have been recently used to obtain three-dimensional images using ultrasonography.
These systems require some discussion in order to properly understand this modality.
Hands-free system
The first system used included a computer capable of classifying images in a given sequence for volume reconstruction upon exploration completion. Images could be rotated around different axes for subsequent reconstruction.
This system, which was employed by Sackman in 1994 (1) for the study of the liver and pancreas, required a prolonged scanning time for the feeding of accurate data into the computer, and relied on the explorer's skills for the obtention of multiple void-free layers. This so-called hands-free system may sometimes include acoustic or magnetic sensors to help position slices for subsequent interpretation.
Mechanical movement system
Systems using mechanical transducers are currently used (VOLUSON 530 and 730, 3-5 MHz, with programs Vocal TM and Shell TM). With these, the explorer no longer needs to obtain slices in a specific sequence or inclination, which besides a certain skill at it demands time. Here the probe itself includes a mechanical movement system for acquiring images to be later processed.
Two types of mechanical transducers exist. One of these transducer types has a mechanical rotating system allowing multiple images to be obtained for subsequent processing by a computer. This system, which lacks the inconveniences associated with manual acquisition, is useful for small anatomic regions, as is the case with endorectal transducers (2).
The other, more advanced mechanical transducer system allows a volume image to be obtained from a truncated cone (VOLUSON 730, 75º scan angle) with its vertex located in the transducer.
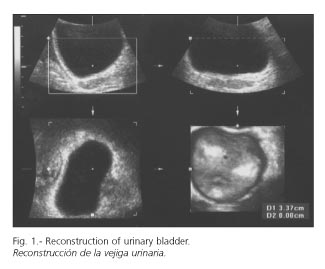
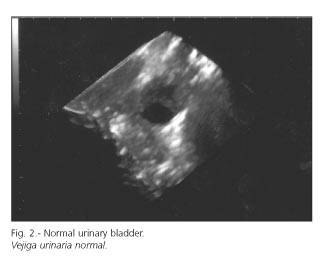
When reaching the region of interest the explorer must keep the transducer stable while the patient stays still, so that the probe may scan two planes simultaneously. Images are then captured and processed by a computer that will display them three-dimensionally (Figs. 1 and 2).
In the multiplanar mode three planes (longitudinal or saggital-A, transverse-B, and coronal-C) and an orthogonal reconstruction are obtained, which may be rotated around three axes (X, Y, Z). The coronal plane may be important for the study of lithiasis at the bladder neck and distal common bile duct, particularly in the presence of a choledochal cyst.
3D color angio and power Doppler scans may also be performed. Vascularization indices, flow, volume, etc., are important.
The multiplanar mode allows visualization of surfaces (surface mode) as well as inner spaces (niche mode).
INDICATIONS IN NON-GASTROINTESTINAL DISEASES
Three-dimensional ultrasonography (3) has now been introduced in selected areas of clinical practice, and thus recent studies demonstrated its usefulness in obstetrics, where this modality seems helpful in diagnosing fetal malformations (4) (hypospadias, cleft lip, spinal malformations, etc.). In the mean time, we should not forget that this technique provides highly realistic fetal images, particularly in slice surface reconstructions and distal portions, which represents a great appeal for parents-to-be (see baby features, etc.). In the field of gynecology, it is mainly used in the diagnosis of uterine malformations (uterine septum) and expansive ovarian lesions -where authors such as Kurjak (5) obtained good results by combining three-dimensional ultrasonography and power Doppler, particularly in the study of the ovarian surface- as well as in the identification of tumor infiltration and the accurate measurement of tumor volumes.
Furthermore, it may detect structural abnormalities in the vessels of malignant tumors -thickening, bending, arteriovenous shunts, microaneurysms, etc.- thus facilitating the lesion's morphologic assessment. Transvaginal transducers have also been used in obstetrics, gynecology, and assisted reproduction settings (6). Conventional transvaginal ultrasounds only allow bidimensional (2D) views of three-dimensional structures. It is expertise that allows the explorer to mentally reconstruct volume from such an image. The possibility of three-dimensional images helps the explorer to this end.
Recent reports in the field of cardiology have shown the significance of this modality for the assessment of heart valves, particularly in the study of mitral function. 3D transthoracic sonography has proven its worth in the diagnosis of congenital heart disorders by providing more detailed information on the mitral valve (7). The study of systolic function has been assessed using angiography, radionuclides, and 3D ultrasonography, and the latter modality was deemed effective in this role (8).
3D sonography has been also assayed in the urologic setting, where it may seemingly detect lithiasis with greater accuracy. A number of reports have shown its usefulness in the study of the ureter using endoluminal probes, which have allowed an in-depth study of ureteric and periureteric anatomy (9). This technique has also been used in the study of expansive vesical and prostatic lesions (Fig. 3), particularly in early stages (10).

A number of studies attempting to assess treatment response in prostate tumors by using 3D ultrasonography and Doppler explorations, which allow flow in the tumor's area to be measured before and after therapy using high-intensity ultrasounds, have shown promising results.
The absence of blood flow in 3D sonograms and power Doppler images reflects the involved tissue following treatment, and accurate volume measurements allow therapy effectiveness to be assessed (11) (Table I).

INDICATIONS IN GASTROINTESTINAL DISEASES
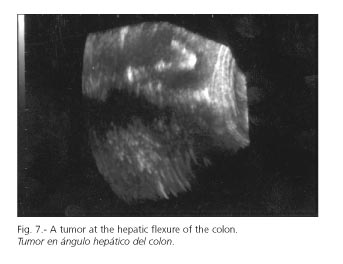
In the field of gastroenterology (12), reports that were first related to this technique evaluated volume measurement accuracy as a future diagnostic potential (13). Clinically, the measurement of volume in an organ or lesion plays a role in the diagnosis and follow-up of multiple diseases. Conventional 2D ultrasonography, which represents a fast, inexpensive way of volume estimation, does so by simply multiplying three perpendicular diameters by 3/4. Obviously, since it is based in the assumption of these geometric figures, this method entails an occasionally significant error margin in volume estimation. Three-dimensional sonography has proven useful at estimating volumes for liver tumors (14) using planimetry, and has shown higher accuracy when compared to conventional 2D sonography and CT, which estimate volume using the ellipse formula (Figs. 4-7).



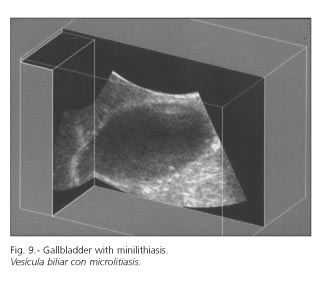
Later on Berstad (15,16) glimpsed a new path for investigation in the study of digestive motility, since it allowed gastric voiding to be assessed as other authors such as Gilja had already demonstrated in 1997 and 1999 (17,18). Subsequent papers such as those by Hausken (19) took advantage of this technique for the measurement of volumes in the assessment of antral and gallbladder emptying in patients with non-ulcerative dyspepsia and in patients with erosive antritis, and they concluded that both antral and gallbladder emptying were abnormal following the ingestion of a test meal. This same author, when studying patients who had dyspeptic symptoms of probably functional nature following cholecystectomy for non-symptomatic biliary lithiasis in comparison to healthy subjects and patients with functional dyspepsia, found overlapping disorders in functional dyspepsia and in patients having undergone cholecystectomy for asymptomatic lithiasis and subsequent dyspeptic symptoms (20) (Fig. 8) .(fig.9)

A step forward for 3D sonography in gastroenterology usage was its application to endoscopic ultrasonography (EUS) (USE) (21), but volumes estimated using this method seem greater than actual.
Thus, Kallimanis (22) reported in 1994 on images obtained from eight patients suffering from esophageal tumors using an Olympus echoendoscope, which were digitalized and then processed in a PC using some software program. Nishimura in 1997 (23) reported his first results: 18 resected tumors in 21 patients. Tumors were esophageal, gastric, and colonic, and their in vitro study yielded surface images similar to gross findings, thus allowing a detailed study of tumor infiltration. Clinical use had limitations, but proved useful in the esophagus and the rectum (24-26).
Some authors have attempted to use three-dimensional sonography in the preoperative study of rectal tumors, and consider this technique useful in their assessment before therapy decision making (27,28). Following intent-to-heal rectal amputation high local relapse rates are known to exist when perirectal fat is infiltrated (29). Furthermore, radiation therapy and chemotherapy increase resectability and survival in advanced tumors. Recent studies have shown that nearly 70% of non-resectable tumors may be eventually excised with healing intent following radiotherapy.
Thus, staging is very important regarding the selection of a proper course of action. The presence of tumor-induced stenosis (14%) has been suggested to be associated with a poor prognosis. However, although stenosing tumors are usually associated with advanced local disease, this is no factor indicating a poor prognosis when considered alone. On the other hand, obstruction alone does not warrant preoperative therapy using radiotherapy and/or chemotherapy. Therefore, in rectal cancer an accurate preoperative assessment is vital, even for tumors inducing no obstruction.
Endorectal sonography is the most accurate technique in the study of rectal cancer thus far. However, this is not possible for stenosing tumors not allowing the passage of a probe through the stenosis. Hünerbein (30) studied 94 consecutive patients with rectal carcinoma. A stenosis was found in 26 that precluded adequate exploration using endorectal sonography; in all these was an endorectal 3D sonogram successful to visualize both the stenosis and the tumor. 3D endosonography successfully diagnosed infiltration extent in 78% of subjects, that is, in 18 patients, and so revealed three patients with an invaded muscularis propria (T2), eight patients with tumors involving perirectal fat (T3), and finally three individuals with invaded nearby organs (T4). Its ability to reveal perirectal lymph node involvement was 75%. Obstruction was correctly attributed to extrinsic lesions developed after surgery in eight patients using 3D ultrasonography. It should be noted that CT had only demonstrated lesions in 6 subjects despite their oscillating between 3 and 6 cm in size. In all eight patients, the diagnosis was confirmed by biopsies performed under the guidance of this same technique.
Another relevant indication of 3D -even 4D (multiplanar real-time visualization)- ultrasonography is in the adjuvant role with interventionist ultrasounds. These results are of great relevance as they demonstrate that this technique is useful to assess infiltration extent even in stenosing tumors (14%) not allowing the passage of a probe, and assessment permits therapy changes in some cases (30,31).
Its usage in the study of pancreatic and biliary diseases has been recently investigated using intraductal probes (32,33); although no definitive results are available yet, this is an appealing path for investigation.
The usefulness (34) of intraductal 3D sonography has been also investigated in the staging of bile duct carcinoma in a small number of subjects. Thus, a series of patients with extrahepatic bile duct carcinoma were preoperatively assessed in a recent paper. All underwent intraductal endoscopic sonography using both conventional and 3D ultrasounds to assess right hepatic artery, portal vein, and pancreatic parenchymal invasion prior to resection. Results were subsequently compared to histological data from resected specimens. Three-dimensional ultrasonography revealed right hepatic artery invasion in 88% of cases, portal vein invasion in 100% of cases, and pancreatic parenchymal invasion 100% of cases, whereas intraductal conventional sonography reached only 88% for all three parameters assessed. Despite the small number of cases studied, these findings allowed authors to conclude that intraductal endoscopic 3D sonography was useful in the staging of bile duct carcinoma.
Finally, some authors such as Kavic (35) maintain that the use of 3D sonography in laparoscopic surgery is glimpsed on the horizon, since it may safely offer precise real-time information on anatomic structures, with no radiation involved and for a relatively inexpensive cost (35,36).
In our setting a review by Weissman in 2001 may be read, in which this author discusses abdominal volumes standardization from 3D sonography (37,38), as well as a more recent review on quantitation (39).
In pediatric patients (3 cases) 3D sonography is an important aid in the diagnosis of grade-I choledochal cysts (40).
CONCLUSIONS
Three-dimensional ultrasonography offers a new perspective into anatomy and pathology, as it allows both the surface and the interior of a lesion to be visualized, and the performance of more accurate volume calculations. It may be of help for all sonography modalities, including interventionist ultrasounds. The future will definitely position this novel technique.
REFERENCES
1. Sackman M, Pauletzky J, Zwiebel FM, Holl J. Three-dimensional ultrasonography in hepatobiliary and pancreatic diseases. Bildgebung 1994; 61: 104-9 [ Links ]
2. Candiani F. The latest in ultrasound: three-dimensional imaging. Part 1. Euro J Radiol 1998; 27 (Supl. 2): 179-82. [ Links ]
3. Campani R, Botinelli O. The latest in ultrasound: three- dimensional imaging. Part II. European Journal of Radiology 1998; 27 (Supl. 2): 183-7. [ Links ]
4. Kurjak A, Vecek N, Hafner T, Bocek T, FunduK KurjaK B, et al. Prenatal diagnosis: what does four-dimensional ultrasound add? J Perinat Med 2002; 30: 57-62. [ Links ]
5. Kurjack A, Kupesic S, Anic T, Kosuta D. Three-dimensional ultrasound and power doppler improve the diagnosis of ovarian lesions. Gynecology-Oncology 2000; 76: 28-32. [ Links ]
6. Maymon R, Herman A, Ariely S, Dreazen E, Buckovsky I, Weinraub Z. Three-dimensional vaginal sonography in obstretics and ginaecology. Hum Reprod Update 2000; 6: 475-84. [ Links ]
7. Lange A, Palka P, Burstow DJ, Godman MJ. Three-dimensional echocardiography: historical development and current applications. J Am Soc Echocardiogr 2001; 14: 403-12. [ Links ]
8. Eder V, Herault S, Hudelo C, Giraideau B, Marchal C, Quilliet L, Pottier J, Arbeille P. Evaluation of left ventricular systolic function by 3D echocardiography: a comparative study with X-ray angiography and radionuclide angiography. Eur J Ultrasound 2000; 11: 105-15. [ Links ]
9. Bagley DH, Liu JB. Three-dimensional endoluminal ultrasonography of the ureter. Journal of Endourology 1998; 12: 411-6. [ Links ]
10. Martino P, Palazzo S, Bufo P, Garofalo L, Selvaggi FP. Three-dimensional ultrasound for early staging of prostatic adenocarcinoma. J Urol 2000; 164: 456. [ Links ]
11. Sedelaar JP, Aarmink RG, Van Leenders GJ. The application of three-dimensional contrast enhanced ultrasound to measure volume of affected tissue after HIFU treatment for localized prostate cancer. Eur Urol 2000; 37: 559-68. [ Links ]
12. Wagner S, Gebel M, Bleck JS, Manns MP. Clinical aplication of 3D sonography in gastrointrestinal disease. Verdauungskrankheiten. 1995; 13: 182-5. [ Links ]
13. Zoller Wg, Liess H. 3D ultrasound in gastroenterology. Bildgebung 1994; 61: 95-100. [ Links ]
14. Liess H, Roth CM, Umgelter A, Zoller WG. Improvements in volumetric quantification of circumscribed hepatic lesions by three dimensional sonography. Zeitschrift für Gastroenterologie 1994; 32: 448-92. [ Links ]
15. Berstad A, Hausken T, Gilja OH, Thune N, Matre K, Odegaard S. Volume measurements of gastric antrum by 3D ultrasonography and flow measurements through the pylorus by duplex technique. Digestive Diseases and Sciences 1994; 39 (Supl. 12): 97S-100S. [ Links ]
16. Berstad A, Hausken T, Gilja OH, Hveem K, Nwsje LB, Odegaard S. Ultrasonography of the human stomach. Scandinavian Journal of Gastroenterology 1996; 220: 75-82. [ Links ]
17. Gilja OH, Detmer PR, Jong JM, Leotta DF, Li XN, Beach KW, et al. Intragastric distribution and gastric emptying assesed by three-dimensional ultrasonography. Gastroenterology 1997; 113: 38-49. [ Links ]
18. Gilja OH, Hausken T, Berstad A, Odegaard S. Measurements of organ volume by ultrasonography. Proceedings of the Institution of Mechanical Engineers 1999; 213: 247-50. [ Links ]
19. Hausken T, Thune N, Matre K, Gilja OH, Odegaard S, Berstad A. Volume estimation of the gastric antrum and the gallbladder in patients with non-ulcer dyspepsia and erosive prepiloric changes, using three-dimensional ultrasonography. Neurogastroenterology and Motility 1994 6: 263-70. [ Links ]
20. Hausken T, Sondenaa K, Svebak S, Gilja OH, Olafsson S, Odegaard S, Soreide O, Berstad A. Common pathogenetic mechanisms in symptomatic, uncomplicated gallstone desease and functional dyspepsia: Volume measurement of gallbladder and antrum using three-dimensional ultrasonography. Digestive Diseases and Sciences 1997; 42: 2505-12. [ Links ]
21. Yoshino J, Nakazawa S, Inui K, Wakabayshi T, Okushima T, Kobayashi T, et al. Surface-rendering imaging of gastrointestinal lesions by three-dimensional ultrasonography. Endoscopy 1999; 31: 541-5. [ Links ]
22. Kallimanis G, Tio TL, Fleisher DE, Benjamin SB. Three dimensional endosonography: a new technique of endoscopic ultrasound. Helenic Journal of Gastroenterology 1994; 7: 217-23. [ Links ]
23. Nishimura K, Niwa Y, Goto H, Hase S, Arisawa T, Hayakawa T. Three-dimensinal ultrasonography of gastrontestinal lesions using an ultrasound probe. Scandinavian Journal of Gastroenterology 1997; 32: 862-8. [ Links ]
24. Hünerbein M, Below C, Schlag PM. Three-dimensional endorectal ultrasonography for staging of obstructing rectal cancer. Diseases of the Colon and Rectum 1996; 39: 636- [ Links ]
25. Hünerbein M, Gretschel S, Ghadimi BM, Schlag PM. Three-dimensional endoscopic ultrasound of the esofagus. Preliminary experience. Surgical Endoscopy 1997; 11: 991-4. [ Links ]
26. Hünerbein M, Ghadimi Bm, Gretschell S, Schalg PM. Three dimensional endoluminal ultrasound: a new method for the evaluation of gastrointestinal tumors. Abdominal Imaging 1999; 24: 445-8. [ Links ]
27. Melchert T, Stroh C, Schramm H. 3D endosonography in the diagnosis of rectal cancer. Coloproctology 1998; 20: 190-7. [ Links ]
28. Ivanov KD, Diacov CD. Three dimensional endoluminal ultrasound: New staging technique un patients with rectal cancer. Diseases of the Colon and Rectum 1997; 40: 47-50. [ Links ]
29. Katsura Y, Yamada K, Ishizawa T, Yoshimaka H, Shimazu H. Endorectal ultrasonography for the assessment of wall invasion and lymph mode metastasis in rectal cancer. Dis Colon Rectum 1992; 35: 362-8. [ Links ]
30. Hünerbein M, Dohmoto M, Haensch W, Schlag PM. Evaluation and biopsy of recurrent rectal cancer using three-dimensional endosonography. Dis Colon Rectum 1996; 39: 1373-8. [ Links ]
31. Lindmark G, Elvin A, Pählmann L, Glimelius B. The value of endosonography in preopoerative staging of rectal cancer. Int J Colorectal Dis 1992; 7: 162-6. [ Links ]
32. Kanemaky N, Nakazawa S, Inui K, Yoshino J, Yamao K, Okushima K. Three-dimensional intraductal ultrasonograhy: Preliminary results of a new technique for the diagnosis of diseases of the pancreatobiliary system. Endoscopy 1997; 29: 726-31. [ Links ]
33. Kanemaky N, Nakazawa S, Inui K, Yosino J, Yamachika H, Okushima K, et al. Three-dimensional ultrasonography using ultrasonic probes by the transpapilary approach for diagnosis of pancreatobiliary diseases. Digestive Endoscopy 1997; 9: 290-95 [ Links ]
34. Tamada K, Tomiyana T, Ohashi A, Wada S, Satoh Y, Miyata T, et al. Properative assessment of extrahepatic bile duct carcinoma using three-dimensional intraductal US. Gastrointestinal Endoscopy 1999; 50: 548-54. [ Links ]
35. Kavic MS. Three dimensional ultrasound. Surgical Endoscopy 1996; 10: 74-6. [ Links ]
36. Bhutani MS. Three dimensional endoscopic ultrasound. Acta Endoscpica 1999; 29: 35-8. [ Links ]
37. Weismann CF, Datz L, Kofler B. Standardized ultrasound (US) 3D-volumen investigation and documentation of the upper abdomen and kidneys. European Radiol 2000; 10: 158. [ Links ]
38. Weismann CF. Utility and application of 3D ultrasound in gastroenterology. Rev Esp Ecogr Dig 2001; 3: 116-20. [ Links ]
39. Fenster A, Downey DB. Three-dimensional ultrasound imaging and its use in quantifying organ and pathology volumes. Anal Bioanal Chem 2003; 377: 982-9. [ Links ]
40. Haliloglu M, Akata D, Gurel S, Ozmen MN, Akhan O. Choledochal cyst in children: evaluation with three-dimensional sonography. J Clin Ultrasound 2003; 31: 478-80. [ Links ]

