










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versão impressa ISSN 1130-0108
Rev. esp. enferm. dig. vol.98 no.4 Madrid Abr. 2006
CARTAS AL DIRECTOR
Mucinous adenocarcinoma on chronic perianal fistula treated by neoadjuvant QT-RT and laparoscopic abdomino-perineal resection
Palabras clave: Adenocarcinoma mucinoso. Fístula perianal. Resección abdómino-perineal.
Key words: Mucinous adenocarcinoma. Perianal fistula. Abdomino-perineal resection.
Dear Director:
Anal carcinoma is an infrequent process and pertains to a rare variant of epithelial neoplasms of the anal channel. Perianal fistula of long evolution is considered a pre-malignant lession. It can be associated with transformation in mucinous adenocarcinoma, habitually difficult to diagnose and associated to a badly forecast (1). Few descriptions in the literature exist nowadays (2).
Case report
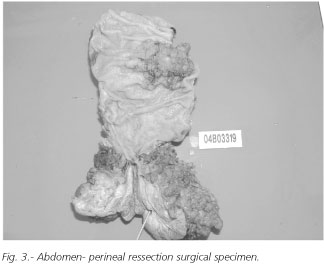
A 62-year-old patient, operated in the last 30 years in three occasions for perianal fistula. In June of 2004 is seen in our Service by presenting perianal fistula with abscess formation, inflammation and fever. He was explored surgically, being obtained scarce quantity of purulent material and, given the ligneous characteristic of the abscess, samples for pathology examination were obtained that were reported as mucinous adenocarcinoma. Colonoscopy showed two tubulo-willous polyps, one of 6 cm of diameter and another of 1 cm located at 12 and 19 cm from anal margin, respectively. Helicoid thoraco-abdominal-pelvic CT scan showed a perineal mass of 5 x 4 cm (Fig. 1), as well as the polyp situated to 12 cm without evidence of lymph node enlargement neither distant metastasis findings what was confirmed by the RMN. With the diagnosis of mucinous adenocarcinoma of perianal fistula or perianal extension of rectal adenocarcinoma, neo-adyuvant chemotherapy was proposed along with radiation therapy of long cycle during 5 weeks and radical surgery thereafter. RT on the pelvis, including tumor with photons -6 MV- and on four isocentric fields complied with Pb to a total dose of 45 Gy in five weeks was administered. The same day chemotherapythe with 5-FU and leucovorin was initiated, cycle that was repeated during the last week of RT. Tumor responded, being reduced its size by 50%. On August 31th, 2004 an abdomino-perineal laparoscopic assisted resection was done. Postoperative period was uneventful. Pathology report was of colloid mucinous adenocarcinoma without lymph node involvement and two adenomas tubulo-villous, the major of them with severe displasia serious (Fig. 2). Patient is free of disease so far in controls.

Discussion
Mucinous adenocarcinoma on chronic perianal fistula constitutes between 3 and 11 percent of all anal carcinomas (3). It can arise de novo or from a cavity of a fistula or abscess. Exact ethiological relation with anal fistula is not established clearly. Upper rectal segment is not found to be affected in reported cases (4). This neoplasm is an aggressive cancer often badly diagnosed and is confusing because of his association to a benign and common disease. If a high index of the suspicion exists biopsy of the fistulous tract is the key for the diagnosis and the early treatment (5). Has been described associated to Paget disease of the anal margin (6).
This neoplasm arises probably from anal glands. Often is presented like an abscess and/or a perianal ffistula. Therefore, the diagnosis often delays. Association with rectal pain and haemorrhage has been described in most of the cases. At the moment of presentation, tumor is habitually over 5 cm in diameter in 80% of the described cases, and the forecast is poor. It produces generally metastasis in inguinal and retro rectal lymph nodes (7).
Endo-rectal ultrasonography CT scan an NMI are fundamental at present for evaluation of the extension of the illness (8).
Recent studies, in the last decade, have shown that locally advanced mucinous adenocarcinoma on perianal fistula would be able to benefit from pre- and postoperative chemo-radiation therapy combined (9). Nevertheless, only isolated descriptions exist. Nevertheless, a complete elimination of the tumor is necessary being abdomino-perineal -classical or laparoscopically assisted- advised and represent the plection procedure associated to inguinal lymphadenectomy according to clinical findings image studies data (10).
In spite of new protocols of therapy, the forecast of mucinous adenocarcinoma of the anal channel on chronic perianal fistula is still poor, owed in its greater part to its advanced nature at the moment of the diagnosis. This reinforces the importance of biopsy of all abscesses and perianal fistulae of chronic evolution for prompt diagnosis and early treatment of the disease (5).
F. J. Ibáñez Aguirre, J. M. Erro Azcárate, F. Aranda Lozano, M. L. Almendral López1,
C. Valenti Ponsa2 and M. Echenique Elizondo3
Departments of Surgery, 1Gastroenterology and 2Pathology. Hospital Zumárraga. País Vasco.
3Department of Surgery. Basque Country University. San Sebastián
References
1. Mates IN, Dinu D, Radulescu G, Iosif C. Infiltrating mucinous carcinoma developed on chronic anal fistula; diagnostic and surgical difficultie. Chirurgia 2003; 98 (5): 459-64.
2. Zbar AP, Shenoy RK. Synchronous carcinoma of the sigmoid colon and a perianal fistula. Dis Colon Rectum 2004; 47 (4): 544-5.
3. Patrinou V, Petrochilos J, Batistatou A, Oneniadum A, Venetsanou-Petrochilou C. Mucinous adenocarcinoma arising in chronic perianal fistulas. J Clin Gastroenterol 2001; 33 (2): 175-6.
4. Dal Bo R, Discalzo L, Conti F, Cimarelli S. Carcinogenic perianal fistula. Minerva Chir 1990; 45 (13-14): 981-2.
5. Marti L, Nussbaumer P, Breitbach T, Hollinger A. Perianal mucinous adenocarcinoma. A further reason for histological study of anal fistula or anorectal abscess. Chirurg 2001; 72 (5): 573-7.
6. Wong AY, Rahilly MA, Adams W, Lee CS. Mucinous anal gland carcinoma with perianal Pagetoid spread. Pathology 1998; 30 (1): 1-3.
7. Erhan Y, Sakarya A, Aydede H, Demir A, Seyhan A, Atici E. A case of large mucinous adenocarcinoma arising in a long-standing fistula-in-ano. Dig Surg 2003; 20 (1): 69-71.
8. Navarra G, Ascanelli S, Turini A, Lanza G, Gafa R, Tonini G. Mucinous adenocarcinoma in chronic anorectal fistula. Chir Ital 1999; 51 (5): 413-6.
9. Anthony T, Simmang C, Lee EL, Turnage RH. Perianal mucinous adenocarcinoma. J Surg Oncol 1997; 64 (3): 218-21.
10. Schaffzin DM, Stahl TJ, Smith LE. Perianal mucinous adenocarcinoma: unusual case presentations and review of the literature. Am Surg 2003; 69 (2): 166-9.

