










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versão impressa ISSN 1130-0108
Rev. esp. enferm. dig. vol.100 no.10 Madrid Out. 2008
Obscure gastrointestinal bleeding due to ileal carcinoid tumor diagnosed by capsule endoscopy
Hemorragia digestiva de origen oscuro por un tumor carcinoide ileal diagnosticado
Palabras clave: Tumor carcinoide de íleo. Sangrado gastrointestinal. Cápsula endoscópica.
Key words: Ileum carcinoid tumor. Obscure gastrointestinal bleeding. Capsule endoscopy.
Dear Editor,
Patients with obscure gastrointestinal bleeding (OGIB) represent 5% of all gastrointestinal bleeding. The culprit lesion is usually located in the small bowel (SB). These patients are often difficult to manage and frequently undergo extensive investigation. Capsule endoscopy (CE) has dramatically changed the evaluation of OGIB (1).
Clinical case
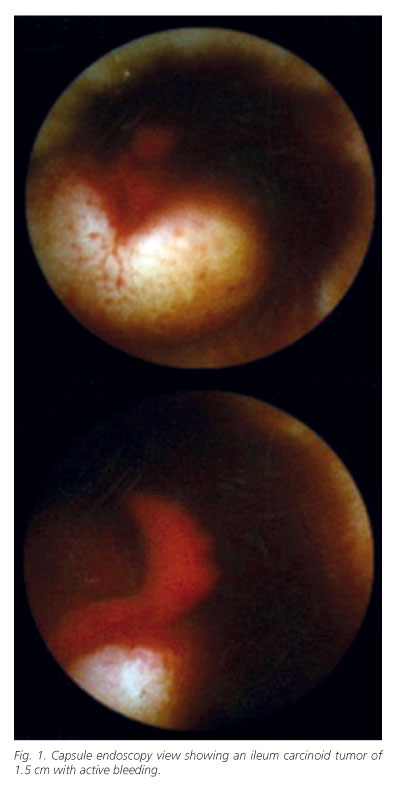
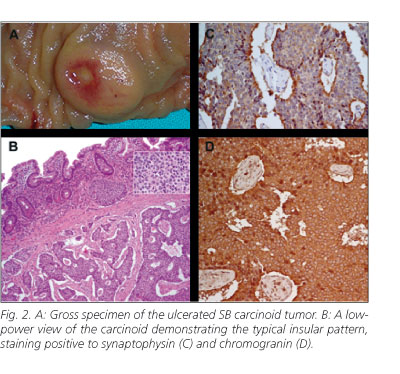
We present a case of a 54-year-old male who was transferred to our hospital with massive hematochezia. He reported previous colonic hyperplasic polyps and sporadic intake of anti-inflammatory for headache. He denied any history of abdominal pain, change in bowel habit, weight loss, previous history of bleeding or other symptoms. Aside from pallor of skin and mucosae no other physical abnormalities were noted. The patient was hemodynamically unstable (blood pressure-92/48 mmHg; heart rate-102 beats per minute), with a haemoglobin-8,2 g/dl and hematocrit-25,4%, and needed 2 units of blood to be stabilized. All other laboratory tests were normal as well as upper endoscopy. Colonoscopy revealed blood clots throughout the entire colon. The following day, colonoscopy with ileoscopy (the last 10 cm) was repeated and no bleeding lesion was identified. Abdominal-pelvic computed tomography did not reveal any abnormality. On the third day of admission, CE was performed and revealed a small rounded lesion in the ileum with a depressed center, which looked like a submucosal tumor with spurting bleeding (Fig. 1). The patient remained hemodynamically stable. On the seventh day of admission, the patient had a planned exploratory laparotomy. A 1.5 cm nodular lesion was found in the ileum, about 70 cm from the ileocecal valve (Fig. 2). No metastases were detected intraoperatively. Segmental ileal and mesentery resection was performed. Histopathologic evaluation, including immohistochemistry study, revealed a carcinoid tumor (1.5 x 1.4 x 0.4 cm) with mucosal ulceration, invading the muscularis propria, but without vascular or regional lymph node invasion (Fig. 2).
Measurements of serum chromogranin A and urinary 5-hidroxyindole acetic were within normal ranges. The patient was discharged after an uneventful postoperative recovery. After a 12 month follow-up, there was no recurrence of haemorrhage and surveillance exams were normal.
Discussion
Incidence of SB tumors is higher than previously reported, with malignancy rates of over 60%. SB tumors are a significant finding at CE (3-9%) (2-4), carcinoid tumors being the most frequent neoplasm (5). These tumors are more common in the ileum and most of them are malignant in nature (5,6). In some cases there may be multiple tumors and other cancers (gastrointestinal tract, lung, cervix, ovaries) are found in 20% of patients, therefore needing appropriate surveillance (5,6).
SB carcinoid tumors in the early stages are usually asymptomatic and conventional diagnostic tests are unreliable (5,6). Diagnosis is frequently delayed, and therefore most of them are disseminated (64.1% of the cases) at diagnosis (5). Transmural invasion and extensive fibrosis are common features contributing to the aggressive behaviour of those tumors (5). SB tumors detected via CE are frequently revealed by OGIB/anemia symptoms (80%) (1,2,4). The yield of clinically important findings on CE in patients with OGIB is 53% and is greater in patients with obscure-overt rather than obscure-occult GI bleeding (60 vs. 46%) (1).
CE has the potential to achieve earlier diagnosis of SB malignancies offering a greater chance of cure. Even in patients with known metastatic disease, CE can alter treatment avoiding the need for further investigation and repeated transfusions, so this tool should be considered at an early stage of investigation for suspected SB disease (1-3). This case highlights the importance of using CE during the initial presentation of occult-overt GI bleeding once the patient is hemodynamically stable. Timing of CE is important because it can have great impact on patient management and outcome (1,2).
V. Costa Dias, J. Soares, G. Villas Boas and M. Santos1
Departments of Gastroenterology and 1Surgery. Hospital Geral de Santo António-Porto. Portugal
References
1. Carey EJ, Leighton JA, Russell I, Shiff AD, Sharma VK, Post JK, et al. A single-center experience of 260 consecutive patients undergoing capsule endoscopy for obscure gastrointestinal bleeding. Am J Gastroentererol 2007; 102: 89-95. [ Links ]
2. ICCE 2006 Conference Report on Capsule Endoscopy. 2006; 1-10. Available at: www.icce.info- [ Links ]
3. Bailey AA, Debinski HS, Appeyard MN, Remedios ML, Hooper JE, Walsh AJ, et al. Diagnosis and outcome of small bowel tumors found by capsule endoscopy: a three-center Australian experience. Am J Gastroenterol 2006; 101: 2237-43. [ Links ]
4. Rey JF, Ladas S, Alhassani A, Kuznetsov K, and the Guidelines Committee. Video capsule endoscopy: up to guidelines. Endoscopy 2006; 38: 1047-53. [ Links ]
5. Modlin IM, Kidd M, Latich I, Zikusoka MN, Shapiro MD. Current status of gastrointestinal carcinoids. Gastroentererology 2005; 128: 1717-51. [ Links ]
6. Ramage JK, Davies AHG, Ardill J, Bax N, Caplin M, Grossman A, et al. Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumors. Gut 2005; 54: i1-iv 16. [ Links ]

