










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versão impressa ISSN 1130-0108
Rev. esp. enferm. dig. vol.101 no.6 Madrid Jun. 2009
PICTURES IN DIGESTIVE PATHOLOGY
Intestinal and biliary infection with Ascaris lumbricoides in gastrointestinal endoscopy
Infección intestinal y biliar por Ascaris lumbricoides en endoscopia digestiva
L. Julián-Gómez, J. Barrio, C. de la Serna, M. Pérez-Miranda, P. Gil-Simón, S. Gómez de la Cuesta, R. Atienza and A. Caro-Patón
Service of Digestive Diseases. Hospital Río Hortega. Valladolid, Spain
Case report 1
A 54-year-old female patient with no relevant history underwent colonoscopy for rectal bleeding. An ascaris worm was seen at the appendiceal orifice, which was withdrawn using a polypectomy snare and sent to microbiology for diagnosis confirmation. Treatment consisted of single-dose albendazole.
Case report 2
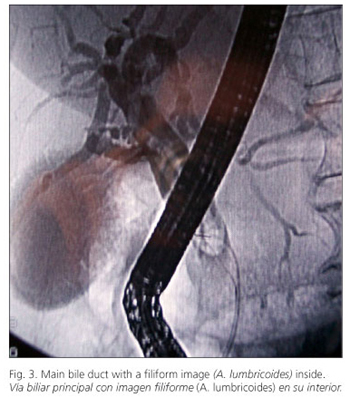
A female patient was admitted because of epigastric pain radiating to the right hypochondrium, associated with nausea and vomiting, over the past 24 hours. Laboratory tests: leukocytosis 137,500/mm3, polymorphonuclear leukocytes 75%, amylase 1956 U/L, AST: 89 U/L, ALT 120 U/L. Abdominal ultrasounds: dilated extrahepatic bile tract with repletion defects. ERCP: dilated common bile duct with a filiform repletion defect folded onto itself, occupying the entire extrahepatic bile tract. The bile tract was cleared using a Fogarty balloon, and a cylindrical, 23-cm-long worm was withdrawn, together with biliary mud and two bile stones smaller than 10 cm in size. The bile tract was flushed with saline, and therapy with oral albendazole 400 mg for 4 days was prescribed. The patient was discharged with no symptoms on the 7th day after admission.


Discussion
Ascaris lumbricoides is the helminth infection that most commonly affects human beings, with a worldwide prevalence of 25%. Transmission ensues from the ingestion of infective eggs. Infection is commonly asymptomatic and may cause nonspecific gastrointestinal complaints and both intestinal (intestinal obstruction from a mass of worms) and extraintestinal (lung, hepatobiliary, neurological) complications. Hepatobiliary involvement with Ascaris is uncommon in our setting, and may result in biliary colic, alithiasic cholecystitis, cholangitis, acute pancreatitis, and liver abscess. Diagnosis results from eggs found in fecal matter or from plain X-ray in intestinal infection or ultrasounds, CT or ERCP in biliary illness. Treatment consists of anti-helminth agents. ERCP is also recommended for helminth removal without sphincterotomy.

Recommended references
1. Khuroo MS. Ascariasis. Gastroenterol Clin North Am 1996; 25: 553-77. [ Links ]
2. Khuroo MS, Zargar SA, Mahajan R. Hepatobiliary and pancreatic ascariasis in India. Lancet 1990; 335: 1503-6. [ Links ]
3. Valentine CC, Hoffner RJ, Henderson SO. Three common presentations of ascariasis infection in an urban Emergency Department. J Emerg Med 2001; 20: 135-9. [ Links ]
4. Cho YD, Kim YS, Cheon YK, Shim CS, Hong SS. Ascaris-induced acute pancreatitis treated endoscopically. Gastrointest Endosc 2007; 66: 1226-7. [ Links ]

