










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.102 no.4 Madrid abr. 2010
PICTURES IN DIGESTIVE PATHOLOGY
Morgagni-Larrey diaphragmatic hernia as cause of intestinal obstruction in a patient with Marfan's syndrome
Hernia diafragmática de Morgagni-Larrey como causa de obstrucción intestinal en una paciente con síndrome de Marfan
L. Martínez-Lesquereux1, P. Parada-González1, F. Macías-García2 and A. Beiras-Torrado1
1Digestive Surgery Department and 2Gastroenterology Department. University Hospital of Santiago de Compostela. A Coruña, Spain
Clinical case
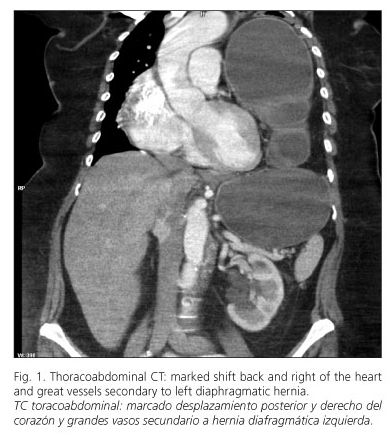
We present the case of a 53-year-old woman with Marfan´s syndrome, who suffered abdominal pain, nausea and vomiting. Laboratory test showed only elevation of leucocytosis (13,450 cells). Chest radiograph revealed the existence of a large air bubble at midthoracic level. Computed tomography (Figs. 1 and 2) revealed the existence of a left diaphragmatic defect at the anterior midline, with partial gastric herniation through it and conditioning a high-grade gastric obstruction. Almost the entire colon and multiple ileal segments were also at intrathoracic position. Following the introduction of a nasogastric tube suction the patient improved significantly, so a scheduled laparoscopic surgery was performed: reduction of viscera into the abdominal cavity and repairing of the left anterior hernial orifice with the placement of prostheses.

Discussion
Congenital diaphragmatic hernia is a rare condition. The so-called hernia of Morgagni (anterior location) is about 3-5% of the diaphragmatic hernias, being the right side the most frequently affected, as the pericardium protects the left side (1). Our case (left anterior congenital diaphragmatic hernia, or Morgagni-Larrey) is, therefore, an entity of exceptional occurrence. The diaphragmatic defect seen in this type of hernia is antero-medially at the junction of the septum transversum of the diaphragm and chest wall (2). The abdominal viscera may not migrate into the chest until late in life, allowing the existence of an asymptomatic diaphragmatic hernia until the development of a complication (3). Surgical treatment is the first option in this pathology, being optional the abdominal or thoracic approach. After reduction of herniated contents into the abdomen, the diaphragmatic defect should be repaired either by primary suture (in cases of small holes) or by the use of a mesh. The laparoscopic approach could be a good option for the management of these patients (3,4).
References
1. Arráez-Aybar LA, González-Gómez CC, Torres-García AJ. Hernia diafragmática paraesternal de Morgagni-Larrey en adulto. Rev Esp Enferm Dig 2009; 101(5): 357-66. [ Links ]
2. Stimec BV, Milisavljevic M, Malikovic A, Fasel JH. Omental Morgagni-Larrey hernia: an anatomical pictorial essay. Clin Anat 2008; 21(6): 587-91. [ Links ]
3. Horton JD, Hofmann LJ, Hetz SP. Presentation and management of Morgagni hernias in adults: a review of 298 cases. Surg Endosc 2008; 22(6): 1413-20. [ Links ]
4. Dapri G, Himpens J, Hainaux B, Roman A, Stevens E, Capelluto E, et al. Surgical technique and complications during laparoscopic repair of diaphragmatic hernias. Hernia 2007; 11(2): 179-83. [ Links ]

