










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.103 n.9 Madrid Sep. 2011
https://dx.doi.org/10.4321/S1130-01082011000900012
LETTERS TO THE EDITOR
Biliopleural fistula after radiofrecuency ablation of hepatocellular carcinoma
Fístula biliopleural tras la ablación con radiofrecuencia de un carcinoma hepatocelular
Key words: Radiofrequency liver. Biliopleural fistula. Pleural effusion.
Palabras clave: Radiofrecuencia hepática. Fístula biliopleural. Derrame pleural.
Dear Editor,
In recent years, percutaneous radiofrequency ablation has emerged as an effective way to treat local primary or metastatic liver tumors. However, it is a procedure that involves quite a lot of complications. We report the case of a biliopleural fistula secondary to radiofrequency ablation of a hepatocellular carcinoma.
Case report
A 76 years old male patient with a history of left hepatectomy and cholecystectomy was diagnosed, in 2001, with hepatocellular carcinoma (HCC) stage A, seven years later. He was treated with percutaneous radiofrequency because of a new HCC in LHD. One month later, the computer tomography (CT) scan showed an effective treatment of HCC and a right pleural effusion less than one third of the hemithorax with no other findings or associated symptoms.
Two months later, he went to the hospital with a right chest pleuritic pain and dyspnea of one week duration. The chest radiograph showed a large right pleural effusion (Fig. 1). Intrathoracic drainage was performed, obtaining a turbid pleural fluid. In the culture, it was isolated an Escherichia Coli that was treated according with antibiotic sensitivity.
The biochemical study of the pleural fluid showed bilirubin 5.2 mg/dL (Bilirubin ratio pleura/serum > 1).
Suspecting a biliopleural fistula, a thoracoabdominal CT was performed, which showed a posterior-basal hydropneumothorax without evidence of fistula.
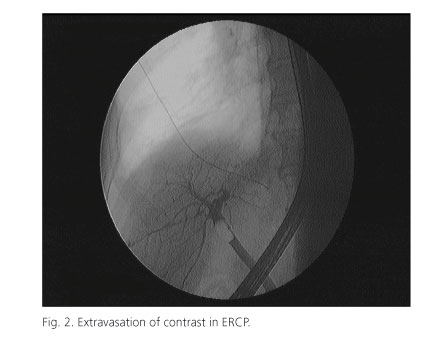
An endoscopic retrograde cholangiopancreatography (ERCP) was programmed, confirming the presence of biliopleural fistula with contrast extravasation into the pleural cavity (Fig. 2). During this procedure was performed a sphincterotomy and placement of a 10 x 12 mm bilioduodenal endoprotesis without incidents.
The biliopleural debit partially decreased, maintaining the fever and persisting in the radiological controls an absence of complete pulmonary reexpansion by pleural thickening.
It was decided then to perform a thoracoscopy, in which we found a blocked cavity by pleural adhesions and basal residual space with not reexpanded right lower lobe. Pleural biopsy and cleaning wall cavity was applied, leaving Pezzer tube tunneled into the skin. The pathological examination of the parietal pleura disclosed an inflammatory tissue without signs of malignancy.
The patient was discharged afebrile, in good general conditions and a minimal, posterior pleural space, maintaining low debit pleural drainage which was successfully removed one month later.
Discussion
The enthusiasm for the treatment of primary and metastatic liver tumors by radiofrequency has grown in recent years, reinforced by its effectiveness and low morbidity. In spite of this, it is necessary to know the possibility of complications associated with this technology.
Complications have been reported secondary to liver radiofrecuency (1) ranging from bleeding (1.6%), intrahepatic abscess (1.1%), and vascular liver or biliary damage (1.7%) to liver failure (0.8%). In less than 1% of these, there are pulmonary complications such as pneumothorax, pleural effusion or hydropneumothorax, and even in minor proportion, biliopleural fistula (0.1%).
In most cases, the biliopleural fistula was resolved with conservative treatment. It combines pleural drainage, antibiotic therapy and sphincterotomy with biliary stenting by ERCP (2-4). This latest technique allows us to decrease the pressure gradient in the Oddi's sphincter, decreasing progressively the fistula output, until its closure in a few days without surgical intervention. There are described cases in which this treatment was associated with somatostatin or octreotide (5).
In some cases, it is not enough with the conservative treatment to solve the pleuropulmonary disease, because of persistent biliary fistula, presence of diaphragmatic lacerations, bronchial fistulas, or need for lung decortication or pleurodesis, that are forcing to realize a thoracoscopy or thoracotomy (2).
Leire Azcarate Perea1, Nicolás Moreno Mata1, Guillermo González Casaurrán1,
Jesús Isea Viña1, Ana M. Matilla Peña2 and Federico González Aragoneses1
Departments of 1Thoracic Surgery and 2Digestive Medicine. Hospital General Universitario Gregorio Marañón. Madrid, Spain
References
1. Curley SA, Marra P, Beaty K. Early and late complications after radiofrecuency ablation of malignant liver tumors in 608 patients. Ann Surg 2004;239:450-8. [ Links ]
2. Lewis JR, Te HS, Gelhbach B, et al. A case of biliopleural fistula in a patient with hepatocellular carcinoma. Nat Rey Gastroenterol Hepatol 2009;6:248-51. [ Links ]
3. Pende Y, Marchese M, Mutignani M, et al. Endoscopic management of biliopleural fistula and biloma alter percutaneous radiofrecuency ablation of liver metastasis. Gastrointest Endosc 2007;66 (33):616-8. [ Links ]
4. Liberale G, Delhaye M, Ansay J, et al. Biliary pleural fistula as a complication of radiofrecuency ablation for liver metastasis. Acta Chir Belg 2004;104:448-50. [ Links ]
5. Lee MT, Hsi SC, Hu P, et al. Biliopleural fistula: A rare complication of percutaneous transhepatic gallbladder drainage. World J Gastroenterol 2007;13(23):3268-70. [ Links ]

