










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.104 no.4 Madrid abr. 2012
https://dx.doi.org/10.4321/S1130-01082012000400013
LETTERS TO THE EDITOR
The mathematics behind the twin-stoma gastrostomy
Las matemáticas detrás de la gastrostomía de estoma doble
Key words: Gastrostomy. Enteral nutrition. Dysphagia. Tube feeding. Stroke.
Palabras clave: Gastrostomía. Nutrición enteral. Disfagia. Alimentación por sonda. ACV.
Dear Editor,
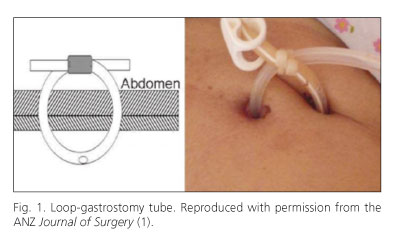
The twin-stoma gastrostomy and the loop-gastrostomy tube are counterparties. They give a fine-bore, secure and easy to exchange feeding tube. We analyze the twin-stoma to get a handle on the loop-tube. The mathematics of the twin-stoma supports the loop-tube as the feeding tube of choice, for all seasons.
The loop-gastrostomy tube is a secure feeding tube because it is locked in position (1). At the same time, it is safe to exchange because the fresh tube is belayed into position by the old (2). The counterparty to a tube is the stoma. We analyze the twin-stoma for a deeper understanding of the loop-tube (Fig. 1).
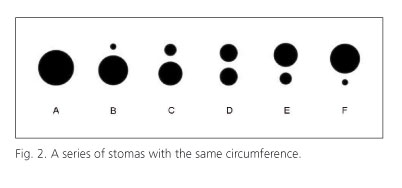
In figure 2, A is a single stoma whereas B, C, D, E and F are pairs of stomas. The combined diameters (d1 + d2) of the two stomas in each pair are equal to the diameter (D) of A. It can be proven that the area of every pair is smaller than A.


Traditionally, the single stoma has been the standard. In the clinical setting, the good doctor inserts a larger-caliber tube which can be deployed, not a smaller-caliber one which is available. This is the default policy, regardless of the technique of insertion (surgical, laparoscopic, endoscopic or radiologic). There are practical reasons for it. First, a larger tube allows a thicker feed to be given. Second, it allows a smoother flow for any given feed. Third, it takes a longer time to clog up. Exchange of tube is thus delayed for a longer period of time.
If the standard tube which results in stoma A is safe, then two tubes which result in B, C, D, E or F are safer. This conclusion is logical because the total area they occupy is smaller. Indeed, clinical experience has confirmed that the smaller-caliber tube has a lower rate of infection (3).
Intuitively, the smallest stoma is preferred by the patient. Of the pairs, D (twin-stoma) has the smallest area, is the most comfortable.
With the twin-stoma, the wise doctor follows a different policy: insert the smallest-caliber loop-tube which can handle the chosen commercial formula, giving maximum comfort to the patient. A blocked tube is no longer an issue because tube exchange is risk-free (2).
In conclusion, the twin-stoma gives a small but useable footprint. This is not the impression many doctors have when they encounter the loop-gastrostomy tube for the first time. Our article hopes to correct the misconception. Clearly, the mathematics underscores it as the feeding tube of choice, regardless of season.
Ah San Pang1 and Soong Kuan Wong2
1LP Surgery. 2The Colorectal Clinic. Mount Alvernia Medical Centre A, Singapore
References
1. Pang AS, Low JM. The twin-stoma gastrostomy. ANZ J Surg 2011;81:575. [ Links ]
2. Pang AS. Risk-free gastrostomy tube exchange. Ann R Coll Surg Engl 2011;93:419-20. [ Links ]
3. Zopf Y, Konturek P, Nuernberger A, Maiss J, Zenk J, Iro H et al. Local infection after placement of percutaneous endoscopic gastrostomy tubes: A prospective study evaluating risk factors. Can J Gastroenterol 2008;22:987-91. [ Links ]

