










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.105 no.2 Madrid feb. 2013
https://dx.doi.org/10.4321/S1130-01082013000200007
PICTURES IN DIGESTIVE PATHOLOGY
Trichotillomania and trichophagia: The causes of Rapunzel syndrome
Tricotlomanía y tricofagia: la causa del síndrome de Rapunzel
Nuno Veloso, João Dinis Silva, Lurdes Gonçalves, Isabel Medeiros, Rogério Godinho and Celeste Viveiros
Gastroenterology Department. Hospital Espírito Santo. Évora, Portugal
Introduction
Trichotillomania, the repeated action of pulling out one's own hair for pleasure or sensation of relaxation, and trichophagia, the result of hair eating, usually precede trichobezoar formation.
In most patients, the trichobezoar is located in the stomach; however, in a few number of patients, the gastric trichobezoar has a tail and extends through the pylorus into the small bowel and may even reach the colon, being titled as Rapunzel syndrome (1).
Case report
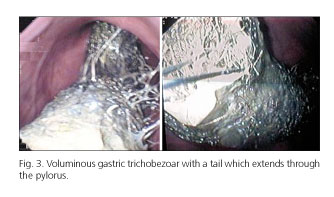
A 7-year-old girl presented to the emergency room with a history of epigastric pain and postprandial emesis over the preceding two days. Physical examination revealed a palpable bulky solid mass, in the epigastric region. Plain abdominal films revealed a mixed density image in the topography of the gastric cavity (Fig. 1). Abdominal ultrasound demonstrated an intragastric hyperechoic rounded solid image (Fig. 2). The final diagnosis was made by upper gastrointestinal endoscopy that showed a voluminous gastric trichobezoar with a tail that extended through the pylorus (blocking visualization) into the duodenal bulb (Fig. 3). An unsuccessful trial was made at endoscopic removal with mechanical and laser fragmentation techniques. Surgical gastrostomy was then performed and the trichobezoar (12.5 x 6 cm) was found with a short tail (1.5 cm) (Fig. 4).



Discussion
Rapunzel syndrome is a rare form of trichobezoar. In the literature, various criteria have been used to classify Rapunzel syndrome, but there is no consensus on its definition. Some authors have defined it as a gastric trichobezoar with a tail that extends through the pylorus (2,3); others describe it as a tail that may extend up to the jejunum or beyond.
Patients may remain asymptomatic for many years and could be misdiagnosed by nonspecific symptoms. The gold standard in the diagnosis is upper gastrointestinal endoscopy. Trichotillomania and trichophagia were only reported after the diagnosis in a focused interview with the parents.
References
1. Vaughan ED, Sawyers J, Scott H. Rapunzel syndrome: An unusual complication of intestinal bezoar. Surgery 1968;63:339-43. [ Links ]
2. Mohanta P, Mukhopadhyay M, Maiti S, Mukhopadhyay B. Trichobezoar in children - an uncommon problem. J Indinan Assoc Pediatr Surg 2004;9:30-2. [ Links ]
3. Singla SL, Rattan KN, Kaushik N, Pandit SK. Rapunzel syndrome - a case report. Am J Gastroenterol 1999;94:1970-1. [ Links ]

