










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.106 n.2 Madrid Feb. 2014
https://dx.doi.org/10.4321/S1130-01082014000200003
Histopathological findings in the oral mucosa of celiac patients
Hallazgos histopatológicos en la mucosa oral de los pacientes con enfermedad celiaca
Elena Bardellini1, Francesca Amadori1, Alberto Ravelli2, Marianna Salemme3, Silvia Lonardi3, Vincenzo Villanacci3 and Alessandra Majorana1
1Dental Clinic, University of Brescia, Brescia, Italy
2Gastrointestinal Pathophysiology and Endoscopy, Spedali Civili, Brescia, Italy
3Department of Pathology, Spedali Civili, Brescia, Italy
ABSTRACT
Background: Celiac disease (CD) is an immune-mediated enteropathy triggered by the ingestion of gluten in genetically susceptible subjects. Although the small intestinal mucosa is the main site of the gut's involvement in CD, other mucosal surfaces belonging to the gastrointestinal tract and the gut-associated lymphoid tissue are known to be affected.
Aim: Assuming that the oral mucosa could reflect the histopathological inflammatory alterations of the intestine in CD patients, this study wishes to assess the pattern of T-cell subsets in the oral mucosa of young adults with CD.
Methods: A group of 37 patients (age range 20-38 years; female: male ratio 28:9) with CD were enrolled. Out of 37 patients, 19 patients (group A) followed a gluten free diet (GFD) -2 patients from less than one year; 6 patients between 1 and 5 years; 11 patients more than 5 years- while 18 patients (group B) were still untreated. Fifteen healthy volunteers (age range 18-35 years, female: Male ratio 11:4) served as controls for the CD patients. Ethical approval for the research was granted by the Ethics Committee. Biopsy specimens were taken from normal looking oral mucosa. The immunohistochemical investigation was performed with monoclonal antibodies to CD3, CD4, CD8, and γδ-chains T cell receptor (TCR).
Results: The T-lymphocytic inflammatory infiltrate was significantly (p < 0.0001) increased in group B (both compared with group A and with the control group).
Conclusion: This study confirms the oral cavity to be a site of involvement of CD and its possible diagnostic potentiality in this disease.
Key words: Oral cavity. Biopsy. Immunohistochemical analysis. T-lymphocyte. Celiac disease. Diet.
Introduction
Celiac disease (CD) is a lifelong immune-mediated disorder triggered by the ingestion of gluten, a protein contained in wheat, rye and barley, in genetically susceptible people (1,2).
The typical form of the disease is a malabsorption syndrome with chronic diarrhea, abdominal pain, distention and weight loss. Atypical forms include extra-intestinal manifestations as iron-deficiency anemia, dermatitis herpetiformis, osteoporosis and osteopenia, recurrent aphtous stomatitis (RAS) and dental enamel defects (DED); silent forms are characterized by absence of symptoms with progressive flattening of intestinal villi and positivity to serological tests while potential forms by absence of symptoms and of histological alterations but positivity to serological tests (3-5). The only treatment of CD is a lifelong adherence to a gluten-free diet (GFD), which usually results in remission (1,2).
CD is strictly linked to a genetic predisposition given by particular human leukocyte antigens (HLA), in particular HLA-DQB1 (DQ2 antigen or DQ8 antigen) (6-10). Further, for the realization of the immune reaction responsible for the disease, it is necessary that the gliadin exceeds the intestinal epithelium and reaches the lamina propria, at the level of which interacts with the tissue transglutaminase giving a reaction of Th1 type, with production of specific cytokines and consequent tissue damage, which is manifested by the histological lesions of the duodenal mucosa, and a reaction of Th2 type, in which there is the activation of B lymphocytes into plasma cells and production of antibodies of the type IgA directed against the gliadin, the endomysium and tissue transglutaminase (6,11-12).
CD diagnosis is currently based, after case identification, on serologic IgA EMA (endomysial antibodies) and IgA anti-tTG (anti-tissue transglutaminase) tests and on a small intestinal biopsy with a minimum of four biopsies (two in the distal duodenum and two in proximal duodenum) (13,14). Recently, a new screening technique based on radioimmunoassay method (RIA) allowing IgA anti-tTG dosage in saliva has been developed (15).
Although the small intestinal mucosa is the main site of the gut's involvement in CD, other mucosal surfaces (such as oral, gastric, rectal, terminal ileum, and esophageal) belonging to the gastrointestinal tract and gut-associated lymphoid tissue (GALT), can also be involved (13). According to literature, gluten-driven T-cell activation can be demonstrated in all these sites. Moreover, the oral cavity could react to ingested gluten in a similar manner to gut mucosa, revealing oral changes when the disease is untreated and an improvement in these changes when CD is treated with a GFD (16).
Assuming that the oral mucosa could reflect the inflammatory changes in the intestine of CD patients, this study aims to assess the pattern of T-cell subsets in the oral mucosa of young adults affected by CD, in particular between newly diagnosed patients and patients following a GFD, and also compared to healthy patients.
Methods
Sample selection
This study was designed as a cross-sectional study. In the period from November 2011 to July 2012, we selected a population of 40 patients, composed by 20 patients with diagnosis of CD and under GFD (group A), consecutively enrolled among patients followed by the Gastroenterology Department of Brescia and 20 patients with diagnosis of CD and still untreated (group B), consecutively enrolled among newly diagnosed patients attending the same department.
Inclusion criteria for the study group were: age major than 18 years; diagnosis of CD; positivity of anti transglutaminase antibodies at diagnosis; good compliance with GFD as judged by an interview with specialist dieticians (only for group A). CD was diagnosed at the Gastroenterology Department of Brescia, according to the criteria of the European Society of Pediatric Gastroenterology, Hepathology and Nutrition (ESPGHAN) on the basis of the presence of the CD-related histological lesions of the duodenum mucosa (17).
Three patients were excluded from the study because they did not give informed consent. Out of 37patients (age range 20-38 years; female: male ratio 28:9) with CD, 19 patients (group A) followed a GFD (2 from less than one year; 6 between 1 and 5 years; 11more than 5 years) while 18 patients (group B) were still untreated.
Fifteen healthy volunteers (age range 18-35 years, female: male ratio 11:4), recruited among patients who attended the Dental Clinic from January 2012 to December 2012, served as controls for the CD patients. Inclusion criteria for the control group were: age major than 18years; negativity of anti-transglutaminase antibodies, no drugs consumption, no gastroenterological diseases, no reactive/ infectious/ immune-mediated or auto-immune/ neoplastic oral mucosal lesions. This study was approved by the Ethics Committee (n.o 1344) of the Faculty of Medicine, University of Brescia, Italy, and informed consent was obtained from all patients.
Buccal samples
Buccal specimens were collected by the same clinician (E.B.). After local anesthesia (mepivacaine and adrenaline 1:100000) a biopsy (6 mm punch) was taken from normal looking buccal mucosa, beneath the occlusal line in the region of the second lower molar. The samples were fixed in formalin (4% formaldehyde in pH 7.2 solution) and routinely processed into paraffin.
Immunohistochemistry and microscopy evaluation of buccal samples
Four micron tissue sections were stained with hematoxylin and eosin for morphological evaluation. Immunohistochemical investigation of T-cell subsets was performed using anti- CD3 (Rb, SP7, 1:100, thermo Scientific, Fremont, CA, USA), -CD4 (Ms, 4B12, 1:40, Thermo Scientific), -CD8 (Ms, C8/144B, 1:30, Dako, Glostrup, Denmark) and -TCR CγM1 (Ms, γ3.20, 1:300, Thermo Scientific). Reactivity was revealed using EnVision (Dako) or NovoLink Polymer (Leica Microsystems, Newcastle upon Tyne, UK) followed by diaminobenzidine (DAB).
Ten HPF (high power fields) of each biopsy were examined in order to evaluate T lymphocytes in inflammatory infiltrate. Nikon eclipse 50i microscope was used (40x objective, 10x eyepiece, 20 mm field of view; HPF = 0,196 mm2). The total T lymphocytes-count was carried out for each case and values were expressed as the mean ± SD.
Duodenal samples
Duodenal sampling was carried out by obtaining six duodenal biopsy samples from each patient. Biopsy specimens, orientated with the luminal side uppermost on Millipore filter paper, were subsequently fixed in 4% formalin, embedded in paraffin, sectioned at 4lm and stained with hematoxylin and eosin. As the duodenal biopsies were performed at the moment of the diagnosis, the duodenal histopathological information in group A were obtained from archived data.
Immunohistochemistry and microscopy evaluation of duodenal samples
Immunohistochemistry for CD3 and CD8 (Dako, Glostrup, Denmark) was carried out in all cases to better identify and quantify intraepithelial lymphocytes. The severity of duodenal histopathological alterations was evaluated according to Marsh-Oberhuber (18) and the new proposed classification by Corazza and Villanacci (19,20). The upper normal limit for intraepitheliallymphocytes was considered 25⁄100 epithelial cells, according to recent criteria (21).
Statistical analysis
Statistical analysis was performed with STATA® for Mac, using ANOVA-test. The results were considered statistically significant when p-value < 0.05.
Results
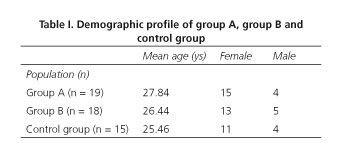
Table I summarizes the demographical profile of the study group and of the control group. The histopathological results are detailed in table II.

Group A (19 patients with CD and following a GFD)
Oral mucosa histopathological findings
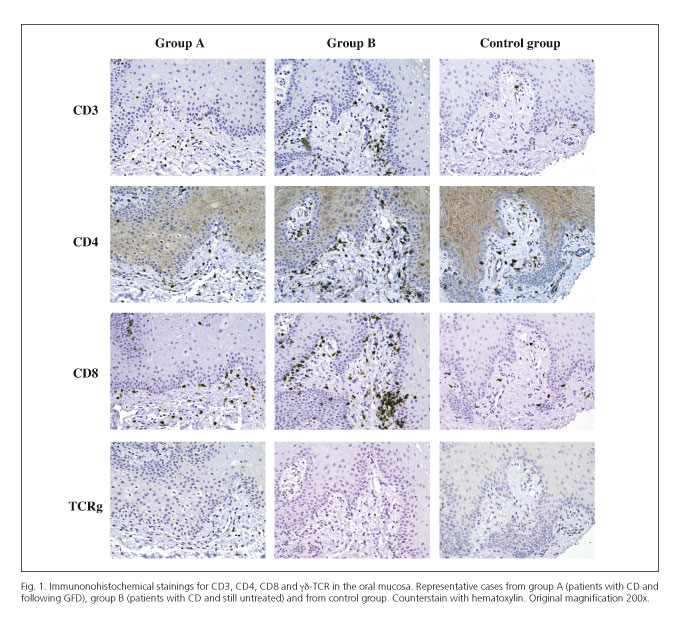
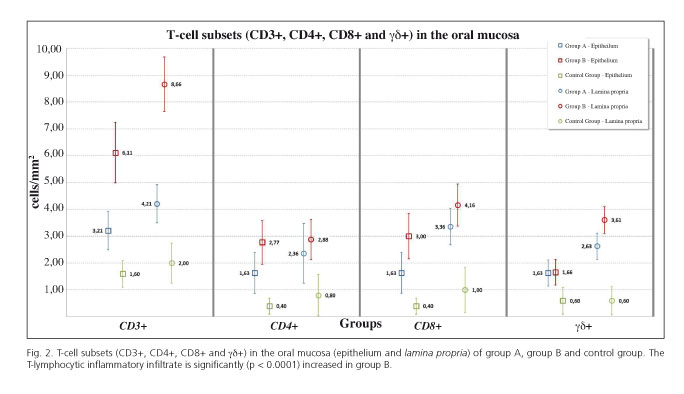
A slight increase of the inflammatory infiltrate was observed if compared with healthy controls but still lower than that in the group B. The staining with hematoxylin-eosin showed absence of epithelial damage, with stromal papillae in which lymphoid cells partly infiltrate the epithelium. Immunohistochemistry analysis performed using monoclonal anti-CD3,-CD4, -CD8 and γδ-TCR (T cell receptor) and showed a lymphocytic inflammatory infiltrate, mainly present at the level of the epithelial-stromal junction (Fig. 1). The presence of CD3 +cells was slightly higher compared to CD4 + and CD8 + cells, but still lower than in group B, especially with regard to CD3 +cells. Even γδ-TCR+ cells were found to be higher than in the control group and slightly lower than those found in group B (Fig. 2). No differences in terms of inflammatory infiltrate were observed respect to the duration of time under GFD.
Duodenal mucosa histopathological findings
While villi architecture was within normal limits, a pathological increase in the number of intraepithelial lymphocytes was observed, besides hyperplastic glandular structures. This is type 2 lesion according to Marsh(22) and to Marsh-modified by Oberhuber (18), or grade A according to the new proposed Corazza and Villanacci classification (19,20).
Group B (18 patients with CD and still untreated)
Oral mucosa histopathological findings
A dense inflammatory infiltrate, especially present at the stromal papillae and rich in lymphoid cells, was observed; a small elongation of the dermal papillae with focal areas of acanthosis and papillomatosis was present. No epithelial damage was found. The immunohistochemical analysis with monoclonal antibodies anti-CD3,-CD4,-CD8 and γδ-TCR, showed, both in the epithelium and in the submucosa, an increase not only of CD3 + cells, mostly represented, but also a dense lymphoid infiltrate composed of CD8 + and CD4 + cells, especially at the level of the epithelial-stromal junction. Moreover, a considerable increase in γδ-TCR+ cells, both at the level of epithelial and of the submucosa was shown (Fig. 1). The T-lymphocytic inflammatory infiltrate was significantly (p < 0.0001) increased both compared with the control group and with group A (Fig. 2).
Duodenal mucosa histopathological findings
Villous atrophy, hyperplastic glandular structures, irregular brush border and pathological increase in the number of intraepithelial lymphocytes were observed. Ten patients showed a type 3 lesion according to Marsh (22) and 3c according to Marsh-modified by Oberhuber (18), or grade B2 according to the new proposed classification of Corazza and Villanacci (19,20); 8 patients showed a type 3 lesion according Marsh (22) and 3b according Marsh modified by Oberhuber (18), grade B1 according to the new proposed classification of Corazza and Villanacci (19,20).
Control group (15 healthy volunteers)
Oral mucosa histopathological findings
A mild T lymphocyte-inflammatory infiltrate, most represented in the submucosa, was observed. The staining with hematoxylin-eosin showed stratified squamous epithelium with normal morphology and architecture, in which a few lymphoid cells scattered mainly at the level of stromal papillae were present. The immunohistochemical analysis showed a lymphocytic infiltrate consisting of CD3 + cells significantly lower than that found in group A and group B (Fig. 1). Similarly, the lymphocyte count of CD4 +, CD8 + and γδ-TCR+ cells was lower in the healthy controls than in group A and group B (Fig. 2).
Discussion
Although nowadays the intestinal mucosa examination is still considered the corner stone for a definitive CD diagnosis, it is known that the disease may affect several extra-intestinal organs, including mucosal surfaces of the gastrointestinal tract and the GALT (13). As the oral mucosa is often involved in CD, it could be considered as a potential site for CD diagnosis; in fact, the oral cavity is easier to access than the small bowel, whose biopsy is often hard to accept, in particular for asymptomatic or mildly symptomatic patients and especially in children.
This study aimed to assess if there are differences in the histological features of the oral mucosa of subjects with CD on GFD, subjects with newly diagnosed CD and healthy controls. Despite the clinical and histological features of CD in the intestine are mostly studied, also the involvement of other mucous membranes belonging to the gastrointestinal tract has been reported (23,24). The activation of T lymphocytes is not only restricted to the proximal part of the intestine, but also at the level of the esophageal and gastric mucosa, of the terminal ileum and of the rectal mucosa.
This study focused on the inflammatory T-lymphocytes infiltrate in the oral mucosa of CD patients compared to healthy subjects. Biopsy specimens of the oral mucosa were taken from three different groups of patients: patients with CD on a GFD (group A), patients with CD still untreated (group B) and healthy controls. Immunohistochemistry analyses were performed by using anti-CD3,-CD4, CD8- and γδ-TCR monoclonal antibodies.
Recent studies (13,25) have shown no differences regarding the B- and T- lymphocyte (including CD3+) counts, both in the epithelium and in the lamina propria of the oral mucosa of CD patients and controls. However the same studies demonstrated that the oral mucosa was unexpectedly affected by spongiosis, probably linked to a local toxic effect which, in turn, was induced by gluten.
According to our results, the T-lymphocytic inflammatory infiltrate was significantly increased in patients with CD still untreated (group B) both compared with patients with CD in GFD (group A) and with the control group. In particular, CD3+ cell counts were significantly higher in group B compared to the other two groups. This could mean that CD3+ T lymphocytes in the oral mucosa correlate with CD activity and its treatment. Again CD4+ and CD8+ cell counts resulted significantly higher in group B than in the other two groups. In a previous study with a similar design, Lähteenoja et al. (16) observed a significant increase in the numbers of mast cells, CD3+ and CD4+ lymphocytes in a group of 44 celiac patients on a GFD but did not find differences in the densities of CD45RO +cells, CD3+ cells or T-cell subsets between 15 untreated CD patients and 19 controls. These slightly different results, compared with our study, may depend on the scarce number of patients of both studies. However, our results seem to reflect what have been shown to happen in the intestinal mucosa, i.e. although a GFD abolishes symptoms, normalizes blood tests and specific serological markers leading to clinical remission, the intestinal mucosa does not fully normalize in all celiac patients in whom a clinical remission is achieved (26); in particular, according to our results, intraepithelial lymphocytes of the duodenal mucosa were more than 25/100 epithelial cells both in group A and group B.
The mucosa of the oral cavity is closely bound to the mucosal-associated surveillance and defense immune system, even if the healthy oral mucosa is immunological different from bowel's one; in fact, the lymphoepithelial structures of Waldeyer's pharyngeal ring in the posterior part of the oral cavity represent an important part of gut-associated lymphoid tissue (GALT) and memory B and T cells migrate to regional lymph nodes and secretory glands after the activation, proliferation and the partial differentiation in GALT. This physiological mechanism probably explains the role of oral mucosa in the immunological pathogenesis of CD.
On the basis of the above histological findings, this study opens new perspectives on CD diagnosis, assessing a histopathological alteration, in terms of lymphocytic infiltrate, in the oral mucosa of CD patients.
Acknowledgments
The authors are grateful to Dr. Clelia Filippini.
References
1. Acar S, Yetkiner A, Ersin N, Oncag O, Aydogdu, Arikan C. Oral findings and salivary parameters in children with celiac disease: a preliminary study. Med Princ Pract 2012;21:129-33. [ Links ]
2. Munoz F, Del Rio N, Sonora C, Tiscornia I, Marco A, Hernandez A. Enamel defects associated with coeliac disease: Putative role of antibodies against gliadin in pathogenesis. Eur J Oral Sci 2012;120:104-12. [ Links ]
3. Abdulkarim AS, Murray JA. Review article: the diagnosis of coeliac disease. Aliment Pharmacol Ther 2003;17:987-95. [ Links ]
4. Rostami-Nejad M, Villanacci V, Hogg-Kollars S, Volta U, Manenti S, Reza-Zali M, et al. Endoscopic and histological pitfalls in the diagnosis of celiac disease: A multicentre study assessing the current practice. Rev Esp Enferm Dig 2013;105:326-33. [ Links ]
5. Reilly NR, Fasano A, Green PH. Presentation of celiac disease. Gastrointest Endosc Clin N Am 2012;22:613-21. [ Links ]
6. Erriu M, Sanna S, Nucaro A, Orrù G, Garau V, Montaldo C. HLA-DQB1 Haplotypes and their relation to oral signs linked to celiac disease diagnosis. Open Dent J 2011;5:174-8. [ Links ]
7. Fernández-Cavada-Pollo MJ, Alcalá-Peña MI, Vargas-Pérez ML, Vergara-Prieto E, Vallcorba-Gómez-Del Valle I, Melero-Ruiz J, et al. Celiac disease and HLA-DQ genotype: Diagnosis of different genetic risk profiles related to the age in Badajoz, southwestern Spain. Rev Esp Enferm Dig 2013;105:469-76. [ Links ]
8. Loeff T, Araya M, Pérez-Bravo F. Frequency of MYO9B polymorphisms in celiac patients and controls. Rev Esp Enferm Dig 2012;104:566-71. [ Links ]
9. Garrote-Adrados JA, Arranz-Sanz E. Genes and populations in susceptibility to celiac disease. Rev Esp Enferm Dig 2012;104:563-5. [ Links ]
10. Piccini B, Vascotto M, Serracca L, Luddi A, Margollicci MA, Balestri P, et al. HLA-DQ typing in the diagnostic algorithm of celiac disease. Rev Esp Enferm Dig 2012;104:248-54. [ Links ]
11. Ludvigsson J, Eylert M, Ilonen J, Vaarala O. Effect of HLA DQ2, dietary exposure and coeliac disease on development of antibody response to gliadin in children. Scand J Gastroenterol 2006;41:919-28. [ Links ]
12. Demarchi M, Carbonara A, Ansaldi N, Santini B, Barbera C, Borelli, et al. HLA-DR3 e DR7 in coeliac disease: Immunogenetic and clinical aspects. Gut 1983;24:706-12. [ Links ]
13. Compilato D, Campisi G, Pastore L, Carroccio A. The production of the oral mucosa of antiendomysial and anti-tissue-transglutaminase antibodies in patients with celiac disease: A review. Scient World J 2010;10:2385-94. [ Links ]
14. Pastore L, Campisi G, Compilato D, Lo Muzio L. Orally based diagnosis of celiac disease: Current perspectives. J Dent Res 2008;87:1100-7. [ Links ]
15. Bonamico M, Nenna R, Montuori M, Luparia RP, Turchetti A, Mennini M, et al. First salivary screening of celiac disease by detection of anti-transglutaminase autoantibody radioimmunoassay in 5000 Italian primary schoolchildren. J Pediatr Gastroenterol Nutr 2011;52:17-20. [ Links ]
16. Lähteenoja H, Toivanen A, Viander M, Räihä I, Rantala I, Syrjänen S, et al. Increase in T-cell subsets of oral mucosa: a late immune response in patients with treated celiac disease? Scand J Immunol 2000;52:602-8. [ Links ]
17. Klapp G, Masip P, Bolonio M, Donat E, Polo B, Ramos D, et al. Celiac disease: The new proposed ESPGHAN diagnostic criteria do work well in a selected population. J Pediatr Gastroenterol Nutr 2013;56:251-6. [ Links ]
18. Oberhuber G, Granditsch G, Vogelsang H. The histopathology of coeliac disease: Time for a standardized report scheme for pathologists. Eur J Gastroenterol Hepatol 1999;11:1185-94. [ Links ]
19. Corazza GR, Villanacci V, Zambelli C, Milione M, Luinetti O, Vindigni C, et al. Comparison of the inter observer reproducibility with different histologic criteria used in celiac disease. Clin Gastroenterol Hepatol 2007;5:838-43. [ Links ]
20. Villanacci V, Ceppa P, Tavani E, Vindigni C, Volta U. Coeliac disease: The histology report. Dig Liver Dis 2011;43:385-95. [ Links ]
21. Ravelli A, Bolognini S, Gambarotti M, Villanaci V. Variability of histologic lesions in relation to biopsy site in gluten-sensitive enteropathy. Am J Gastroenterol 2005;10;177-85. [ Links ]
22. Marsh MN. Grains of truth: Evolutionary changes in small intestinal mucosa in response to environmental antigen challenge. Gut 1990;31:111-4. [ Links ]
23. Alsaigh N, Odze R, Goldman H, Antonioli D, Ott MJ, Leichtner A. Gastric and esophageal intraepithelial lymphocytes in pediatric celiac disease. Am J Surg Pathol 1996;20:865-70. [ Links ]
24. Ensari A, Marsh MN, Loft DE, Morgan S, Moriarty K. Morphometric analysis of intestinal mucosa. Quantitative histological and immunocytochemical studies of rectal mucosae in gluten sensitivity. Gut 1993;34:1225-9. [ Links ]
25. Campisi G, Compilato D, Iacono G, Maresi E, Di Liberto C, Di Marco V, et al. Histomorphology of healthy oral mucosa in untreated celiac patients: Unexpected association with spongiosis. J Oral Pathol Med 2009;38:34-41. [ Links ]
26. Bardella MT, Velio P, Cesana BM, Prampolini L, Casella G, Di Bella C, et al. Coeliac disease: A histological follow-up study. Histopathology 2007;50:465-71. [ Links ]
![]() Correspondence:
Correspondence:
Elena Bardellini
Dental Clinic. P.le Spedali Civili 1, 25133 Brescia, Italy
e-mail:
bardelena@libero.it
Received: 02-12-2013
Accepted: 03-02-2014

