










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.106 no.5 Madrid may. 2014
LETTERS TO THE EDITOR
Metastasis of lobular breast carcinoma in the sigmoid colon
Metástasis de carcinoma mamario lobulillar en sigma
Key words: Lobular carcinoma. Sigmoid metastases. Breast.
Palabras clave: Carcinoma lobulillar. Metástasis sigma. Mama.
Dear Editor,
Metastases of breast carcinomas are usually found in the lung, central nervous system, bone, and liver (1,2). Few cases of colonic metastases from breast cancer have been reported, and the non-specific presentation and variable radiological findings in these cases make diagnosis difficult (2,3).
Case report
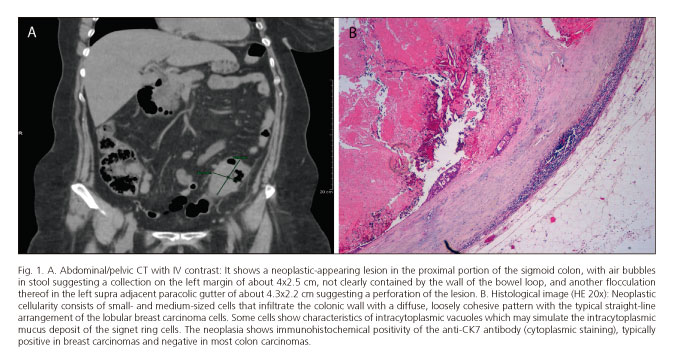
We present a case of metastatic breast cancer in the sigmoid colon: A 69-year-old woman with a history of modified radical mastectomy (MRM), followed by adjuvant chemotherapy, performed 18 years ago (1994) by infiltrating the lobular carcinoma in the right breast. She attended the emergency room for abdominal pain, which over 48 hours became associated with nausea, vomiting and lack of flatulence. The physical examination showed abdominal distension and generalized pain with signs of peritoneal irritation. Laboratory tests showed a discrete leukocytosis (13.62x103). The emergency abdominal/pelvic CT scan with IV contrast showed a lesion with a neoplastic appearance in the proximal portion of the sigmoid colon, with imaging suggesting a collection of about 4x2.5 cm on the left margin, and another of about 4.3x2.2 cm in the left supra adjacent paracolic gutter. The latter had a hydro-aerobic aspect suggesting a perforation of the lesion (Fig. 1A). Given the findings described, emergency surgery was performed during which was observed fecal peritonitis secondary to neoplastic perforation of the sigmoid colon. A sigmoidectomy and end colostomy were performed in the left flank. During the postoperative period, the patient recovered favorably and was discharged from the hospital seven days after surgery. The subsequent anatomopathological study of the tumor showed metastasis of the carcinoma that was poorly differentiated and compatible with the primary breast carcinoma (Fig. 1B). The neoplasia presented immunohistochemistry negative for estrogen receptors, progesterone and HER-2/neu (Hercep test), showing positive for the anti-CK7 antibody usually present in breast carcinomas and absent in most colon carcinomas. The patient underwent postoperative systemic chemotherapy and has remained asymptomatic and disease-free one year after surgery (negative PET-CT during follow-up). At present, she is awaiting bowel reconstruction surgery.
Discussion
Diverse studies have examined the pattern of dissemination of the different histological subtypes - the gastrointestinal, osseous or gynecological disseminations being more frequent in lobular subtypes, and the central nervous system, liver, and lung metastases in ductal subtypes (4). Despite the high prevalence of infiltrating ductal carcinoma, infiltrating lobular breast carcinoma is responsible for most gastrointestinal tract metastases (4-6). Multiple lesions, unilateral defects and extrinsic conditions with healthy mucosa are suggestive signs of metastasis (5-7). Colonoscopy with biopsy is the test of choice to differentiate metastases and primary colonic tumors (4,5,7). An intact mucosa with serous membrane invasion by tumor cells histologically identical to those of the primary breast tumor confirms the diagnosis of metastasis (7). Using immunohistochemical techniques is useful when doubts exist over origin of the tumor and the appropriate adjuvant treatment (chemotherapy and/or hormonal therapy) (8-10). There is no consensus on the management of these uncommon lesions (4). Surgical treatment is reserved for cases of perforation, hemorrhage or intestinal obstruction (4,5).
Jacob Motos-Micó, Manuel Ferrer-Márquez, Ricardo Belda-Lozano,
Ángel Reina-Duarte and Rafael Rosado-Cobián
Department of General Surgery and Digestive Diseases. Hospital Torrecárdenas. Almería, Spain
References
1. Nikkar-Esfahani A, Kumar B, Aitken D, Wilson R. Metastatic breast carcinoma presenting as a sigmoid stricture: Report of a case and review of the literature. Case Rep Gastroenterol 2013;7:106-11. [ Links ]
2. Xiao-Cong Z, Hong Z, Ying-Hai Y, Xiu-Feng Z, Yi J. Invasive ductal breast cancer metastatic to the sigmoid colon. World J Surg Oncol 2012;10:256. [ Links ]
3. Bamias A, Baltayiannis G, Kamina S, Fatouros M, Lymperopoulos E, Agnanti N, et al. Rectal metastases from lobular carcinoma of the breast: Report of a case and literature review. Ann Oncol 2001;12:715-8. [ Links ]
4. Michalopoulos A, Papadopoulos V, Zatagias A, Fahantidis E, Apostolidis S, Haralabopoulos E, et al. Metastatic breast adenocarcinoma masquerading as colonic primary. Report of two cases. Tech Coloproctol 2004;8(Supl. 1):135-7. [ Links ]
5. Thérauxa J, Bretagnola F, Guedjb N, Cazals-Hatemb D, Panis YA. Colorectal breast carcinoma metastasis diagnosed as an obstructive colonic primary tumor. A case reportand review of the literature. Gastroenterol Clin Biol 2009;33:1114-7. [ Links ]
6. Taal BG, den Hartog Jager FC, Steinmetz R, Peterse H. The spectrum of gastrointestinal metastases of breast carcinoma: II. The colon and rectum. Gastrointest Endosc 1992;38:136-41. [ Links ]
7. Dhar S, Kulaylat MN, Gordon K, Lall P, Doerr RJ. Solitary papillary breast carcinoma metastasis to the large bowel presenting as primary colon carcinoma: Case report and review of the literature. Am Surg 2003;69:799-803. [ Links ]
8. McLemore EC, Pockaj BA, Reynolds C, Gray RJ, Hernandez JL, Grant CS, et al. Breast cancer: Presentation and intervention in women with gastrointestinal metastasis and carcinomatosis. Ann Surg Oncol 2005;12:886-94. [ Links ]
9. Arslan C, Sari E, Aksoy S, Altundag K. Variation in hormone receptor and HER-2 status between primary and metastatic breast cancer: review of the literature. Expert Opin Ther Targets 2011;15:21-30. [ Links ]
10. Weigelt B, Peterse JL, Van't Veer LJ. Breast cancer metastasis: Markers and models. Nat Rev Cancer 2005;5:591-602. [ Links ]

