










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 n.2 Madrid Feb. 2015
Infectious etiology of diarrheas studied in a third-level hospital during a five-year period
Etiología infecciosa de las diarreas estudiadas en un hospital de tercer nivel durante un periodo de cinco años
Antonio Damián Sánchez-Capilla1, Antonio Sorlózano-Puerto2, Javier Rodríguez-Granger3, Antonio Martínez-Brocal3, José María Navarro-Marí3 and José Gutiérrez-Fernández2,3
1 Department of Gastroenterology. Hospital Universitario Virgen de las Nieves. Granada, Spain
2 Department of Microbiology. Biohealth Research Institute (Instituto de Investigación Biosanitaria) ibs. GRANADA. Faculty of Medicine. Universidad de Granada. Granada, Spain
3 Department of Microbiology. Biohealth Research Institute (Instituto de Investigación Biosanitaria) ibs. GRANADA. Hospital Universitario Virgen de las Nieves. Granada, Spain
ABSTRACT
Introduction and objective: Infectious diarrheas are highly frequent and responsible for a major consumption of resources. This study identified the main diarrhea-causing microorganisms in a health area of Granada (Spain) and determined changes in the epidemiologic pattern over a five-year period.
Material and method: A retrospective study was conducted based on results obtained in the Microbiology Laboratory of Hospital Universitario Virgen de las Nieves (Granada, Spain).
Results: Out of the 25,113 stool microbiological and/or parasitological studies ordered, 2,292 microorganisms were identified in 2,152 samples from 1,892 patients. There was a predominance of bacterial diarrheas (50.1 %), mainly caused by Campylobacter spp. (22.2 %), whose frequency increased significantly during the last two years, and by Salmonella spp. (16.4 %), whose frequency remained stable during the whole study period. We highlight the high frequency of Rotavirus (33.5 %), although a significant decrease was observed during the last two years. Salmonella spp. was more frequently detected during the summer and autumn, Campylobacter spp. during the spring, and Rotavirus during the winter. Viral processes were predominant (53.3 %) in pediatric patients, mainly Rotavirus in under 2-yr-olds, whereas bacterial processes predominated in older children and adults. Diarrhea began at community level in 84.2 % of patients, requiring hospitalization in 25.8 % of cases, and diarrhea was nosocomial in the remaining 15.8 %.
Conclusions: During the study period, there was a significant increase in the frequency of diarrhea caused by Campylobacter spp., a significant reduction in the frequency of diarrhea due to Rotavirus, and no change in the frequency of diarrhea due to Salmonella spp., all of which showing a marked seasonal distribution.
Key words: Diarrhea. Rotavirus. Campylobacter spp. Salmonella spp.
RESUMEN
Introducción y objetivo: las diarreas infecciosas son muy frecuentes y generan un importante consumo de recursos. Se determinaron los principales microorganismos productores de diarrea en un área sanitaria de Granada y la evolución del patrón epidemiológico durante cinco años.
Material y método: se realizó un estudio retrospectivo a partir de los resultados obtenidos durante cinco años en el Laboratorio de Microbiología del Hospital Virgen de las Nieves.
Resultados: de 25.113 solicitudes de estudio microbiológico y/o parasitológico en heces, se identificaron 2.292 microorganismos, en 2.152 muestras de 1.892 pacientes. Predominaron las diarreas bacterianas (50,1 %), sobre todo por Campylobacter spp. (22,2 %), cuya frecuencia aumentó significativamente en los dos últimos años, y Salmonella spp. (16,4 %), que se mantuvo a lo largo del periodo. Destacó la elevada frecuencia de Rotavirus (33,5 %), aunque disminuyó significativamente en los dos últimos años. Salmonella spp. se detectó más frecuentemente en verano y otoño, Campylobacter spp. en primavera y Rotavirus en invierno. En los pacientes pediátricos predominaron los procesos víricos (53,3 %), destacando Rotavirus en menores de 2 años, mientras que, en niños mayores y adultos, lo hicieron los procesos de origen bacteriano. En el 84,2 % de los pacientes la diarrea se inició a nivel comunitario, siendo necesario el ingreso del 25,8 %, y en el 15,8 %la diarrea fue nosocomial.
Conclusiones: durante el periodo analizado se produjo un incremento significativo de la frecuencia de diarreas por Campylobacter spp., y una disminución, también significativa de Rotavirus, manteniéndose la frecuencia de diarreas por Salmonella spp., todas ellas con una marcada distribución estacional.
Palabras clave: Diarrea. Rotavirus. Campylobacter spp. Salmonella spp.
Introduction
Infectious diarrhea is a clinical situation experienced by most humans on one or many occasions throughout their lives. Although usually self-limiting, with scant local or systemic repercussion, it can occasionally produce an important clinical deterioration that requires specific therapeutic measures or hospitalization and can even, in the most severe cases, end in the death of the patient. It represents a major public health problem responsible for elevated health costs and resource consumption in both primary and hospital care (1,2).
The characteristics of the diarrhea and the clinical situation of the affected individual largely depend on the pathogen involved and patient-related factors, such as age, immune response capacity, mucosal structure, and gut microbiota (3). The most frequently involved microorganisms are: bacteria, such as Salmonella spp., Campylobacter spp., Yersinia spp., Shigella spp., Aeromonas spp., Escherichia coli, Listeria monocytogenes, Staphylococcus aureus, Bacillus cereus, Clostridium difficile, or Clostridium perfringens, among others; viruses, such as Rotavirus, Norovirus or Adenovirus; and protozoa, such as Giardia lamblia, Cryptosporidium parvum, Isospora belli, Entamoeba histolytica, or Cyclospora cayetanensis.
The digestive transmission of these microorganisms from the intake of contaminated food or water and their interpersonal transmission are responsible for outbreaks or epidemics, although most cases of diarrhea are sporadic. It is difficult to establish the true incidence of infectious diarrhea, because it is a self-limiting process and not all patients seek medical care for this condition (4). Moreover, microbiological studies are not always conducted and, when performed, do not always identify the pathogen (2). Although the main treatment, based on oral rehydration measures, is often adequate, some situations require specific antimicrobial treatment (1). This should be prescribed as a function of the clinical status of the patient and the microorganisms most frequently involved in the etiology of the process in each geographic area.
The objective of this study was to identify the main microorganisms causing infectious diarrhea in our setting between 2007 and 2012 and establish their relative frequency and distribution according to the sex and age of patients, the origin of the sample or ordering department, and their annual and seasonal time course.
Material and method
A retrospective descriptive study was conducted using the data from the MicrobDynamic laboratory information system (Francisco Soria Melguizo, SA, Madrid, Spain) of the Microbiology Department of the Hospital Universitario Virgen de las Nieves (Granada, Spain) on the results of microbiological and/or parasitological diagnostic tests of stool samples from patients with episodes of diarrhea and/or non-acute abdominal pain, ordered between October 1, 2007 and September 30, 2012. The hospital complex comprises three hospitals (General/Specialty Hospital, Maternity/Child Hospital, and Traumatology and Rehabilitation Hospital) that meet the demands of the North Hospital Area of Granada province, which includes the Primary Care Health Districts of North Granada, Santa Fe, and Guadix and the Basic Health Area of Alcalá la Real (Jaén, Spain), serving a reference population of around 440,000 inhabitants.
Figure 1 depicts the process of recovering data from the registry of microbiological samples. Searches of the laboratory information system yielded the results of all tests conducted in stool samples during the study period. Those with negative results were excluded (reported at the time as "no enteropathogenic bacteria detected", "negative antigen detection", "absence of fresh parasitic forms", or "absence of acid-fast organisms"): We only selected those with positive microbiological and/or parasitological results, i.e., indicating the presence of the microorganism (bacteria, virus, or parasite) detected and identified in the sample and therefore considered as etiologically responsible for the clinical process motivating the request for the study.
A specific database was designed to collect relevant information based on the positive results selected. Data were gathered on: The affiliation of each patient (by clinical record number and his/her initials), dates of the reception of the sample and the emission of the report of the results, demographic variables (age, sex, and place of residence), outpatient or hospital origin of the sample (and, in the latter case, the department in which the patients were hospitalized), and, finally, the microorganism(s) identified. In order to avoid inclusion bias in the positive results, a control of duplicates was performed by using the clinical record number and initials of patients. In cases in which there was more than one positive result for a single patient, we ruled out studies with an interval of less than 7 days between the reception of the stool sample and the emission of a previous report and with the same microbiological and/or parasitological result, which were considered duplicate or control studies.
Next, the Integrated System of Management and Information for Health Care in Andalusia (Spanish initials, DIRAYA) was used to review the digitalized clinical records of the selected patients and collect clinical data (presence of abdominal pain, dehydration, neurological disorders, or fever, characteristics of the stool, duration of the episode, and days of hospital stay, when appropriate), personal history of interest, hospital or community origin of the diarrhea (considered of hospital/nosocomial origin when the onset was more than 72 h after hospital admission or less than 72 hours after hospital discharge), and other analytical data.
Non-parametric statistical tests were applied. Binomial tests were used to compare the detection frequency of each microorganism as a function of the patients' sex and age; and the Kruskal-Wallis and Mann-Whitney U tests were used to compare the length of hospital stay as a function of the etiology of the clinical process, to evaluate changes in the annual and seasonal distribution of each microorganism, and to establish the possible association of these changes with temporal variations in the number of microbiological and/or parasitological studies ordered. SPSS 18.0 software was used for the statistical analysis. P<0.05 was considered significant in all tests.
Results
Description and distribution of the microorganisms identified
Out of a total of 25,113 requests for microbiological and/or parasitological studies during the five-year study period, 2,292 clinically relevant microorganisms were identified in 2,152 stool samples from 1,892 different patients, yielding an accumulated 5-year incidence of 430 cases/100,000 inhabitants in the reference population. According to these results, an average of around one study in ten yielded a positive result, with a mean of 38 microorganisms identified per month from a mean of around 419 requests per month. Table I shows the distribution of these microorganisms by genus and species and their percentage with respect to the number of requests for microbiological and/or parasitological study for each type of microorganism.

We identified 1,149 bacteria (50.1 % of all microorganisms) from 15,062 requests for stool culture or C. difficile toxin detection by immunochromatography, giving a diagnostic performance of 7.6 positive results per 100 studies conducted. The best-performing diagnostic procedure was the detection of viruses in stool samples, with 1,001 viruses (43.7 % of identified microorganisms) being identified out of 3,049 requests, a mean of 33 positive results per 100 studies conducted. The detection of parasites was the worst-performing procedure, with 142 (6.2 %) being identified out of 7,002 requests, an average of 2 positive results per 100 studies conducted.
Although there was a predominance of bacterial diarrheas, especially those caused by Campylobacter spp. (n = 509; 22.2 %) and Salmonella spp. (n = 377; 16.4 %), we highlight the elevated relative frequency of Rotavirus (n = 768; 33.5 %). Among the parasites, only G. lamblia, Entamoeba coli, E. histolytica, Endolimax nana, and Cryptosporidium spp. were detected in patients with diarrhea; the remaining parasites were identified in patients with non-specific abdominal discomfort or non-acute abdominal pain. A single microorganism was identified as responsible for the clinical process in 2,017 samples (93.7 %), while more than one microorganism was detected in 135 samples, most frequently a combination of two viruses (85 samples), notably Rotavirus-Adenovirus (78 cases). In 110 patients, the same microorganism was detected in two or more samples obtained with an interval of more than one week.
Distribution of infections according to the sex and age of patients
Among the 1,878 patients for whom sex was recorded (99.3 % of the total study sample), 53.0 % were males. Bacterial and viral infections were significantly more frequent in males (53.2 % vs. 46.8 %, p = 0.031; and 54.7 % vs. 45.3 %, p = 0.003; respectively), whereas parasitizations were more frequent in females (58.7 % vs. 41.3 %, p = 0.045).
Among the 1,851 patients (97.8 %) for whom the age was recorded, the mean age was 14.9 ± 24.5 yrs (ranging from 1 month to 100 yrs); 75.5 % of patients were under-14-yr-olds, and the under-2-yr-old age range was the most frequent (47.1 %). Among the infants, there was a higher frequency of viral (53.3 % of cases) versus bacterial (41.9 %) and parasitical (4.8 %) cases, although the classification by age ranges showed that this predominance was largely attributable to the high frequency of viral diarrhea due to Rotavirus in the under-2-yr-olds, with bacterial infections being more frequent at older ages. Among the adults, bacterial infections were significantly more frequent than the other etiologies considered together in all age ranges (78.2 % vs. 21.8 %, p < 0.001).
Differences in the origin of the sample and department ordering the study
Out of the 2,149 cases (99.9 %) for which the origin of the sample was recorded; 44.4 % derived from primary or specialized care outpatient departments, 34.6 % from hospital departments, and 20.1 % from the emergency area. therefore, most (64.5 %) of the microorganisms identified were from outpatient samples. In addition, 0.9 % of samples were from other hospitals -Hospital Provincial San Juan de Dios (Granada, Spain), Hospital de Alta Resolución de Alcalá la Real (Granada, Spain), and Complejo Hospitalario de Jaén (Jaén, Spain). The clinical samples in which bacteria and parasites were identified were mainly from outpatient departments, while the samples in which viruses were identified were mainly from hospital departments, notably the Pediatrics Department. Samples of under-2-yr-old patients were most frequently from hospital departments (Pediatrics, Pediatric ICU, or Pediatric Surgery), whereas those from older children were mainly from outpatient departments. Samples from adult patients aged between 15 and 44 yrs were most frequently from outpatient departments, especially from Primary Care and Gastroenterology Departments, while samples from older patients were most frequently from hospital departments.
Out of the 1,811 (95.7 %) patients for whom the origin of the clinical process was recorded, it was community acquired in 1,525 patients (84.2 %), 393 (25.8 %) of whom required hospitalization, and it began during a previous hospitalization for a reason other than diarrhea or after hospital discharge in the other 286 patients (15.8 %). In both cases, the clinical process was nosocomial diarrhea, and it was an intercurrent process in 56 % of these patients. The diarrheas most frequently requiring hospitalization were those of viral origin (> 50 %) and, in all cases, more than half of the admissions were intercurrent. The mean hospital stay was 6.2 ± 6.5 days for the 393 patients requiring hospitalization, all as a consequence of diarrhea, but was 25.2 ± 38.1 days for those with intercurrent diarrhea (17 ± 15.3 days when the 26 patients with extreme hospital stays > 70 days are not considered).
Table II summarizes the main demographic and epidemiologic data associated with the most frequently identified microorganisms. Diarrheas caused by Campylobacter spp., Rotavirus, and Adenovirus were significantly more frequent in males versus females, with no gender differences in those produced by Salmonella spp. or G. lamblia. Moreover, they were all (except for those produced by G. lamblia) significantly more frequent in under-14-yr-old children, especially the viruses, as commented above. In most cases, the samples were of community origin (Primary Care and Specialized Care Outpatients), given that in more than 75 % of cases, according to the etiology, the clinical process began at outpatient level and did not require hospitalization (except in the case of diarrhea due to Rotavirus, with around half of the samples coming from hospitalization rooms in the Pediatric Department, despite their more frequent outpatient onset, given the need for the hospitalization of patients as a consequence of the clinical course).
When the diarrhea was caused by any of these microorganisms (Table II), the mean hospital stay was longer when the clinical process was caused by G. lamblia (23.3 days ± 21.2), Campylobacter spp. (22.3 days ± 47), or Rotavirus (20.5 days ± 43.5). However, there were no statistically significant differences (p > 0.05 in all cases) in hospital stay among these etiologies or in comparison to others, such as Salmonella spp. (10.1 days ± 19) or Adenovirus (18.9 days ± 27.3).
Annual and seasonal distribution of infectious diarrheas
Finally, we analyzed the annual (considering periods between October and September) and seasonal distribution of the number and type of microorganisms identified in relation to temporal variations in the number of requests for microbiological and/or parasitological studies of stool samples during the study period. A significant increase (p = 0.016) was observed in the detection of bacteria during the last two years, which was not a consequence of the increase in requests, which remained stable and with no seasonal variations. Considering only the most frequently identified bacteria (Fig. 2A), it can be observed that the frequency of Campylobacter spp. significantly increased during the last two years in comparison to the rest of the study period (p = 0.029), with more than double the number of cases during the last year with respect to the first three years, while cases of Salmonella spp. (and of other bacteria) remained stable during the study period. The seasonal distribution of these bacteria (Fig. 2B) showed that Salmonella spp. was more frequently detected during the summer and autumn and Campylobacter spp. during the spring. Moreover, there were peaks of higher relative frequency of bacterial diarrheas in June 2008, May 2011, September 2011, and August 2012.
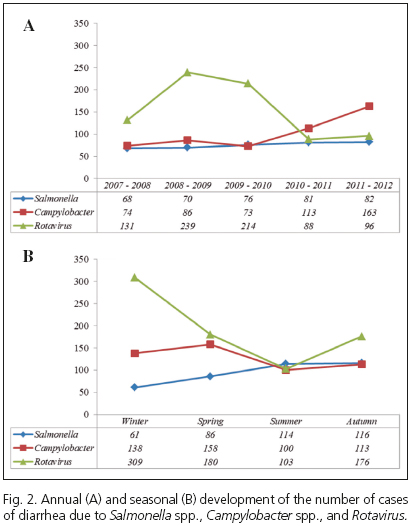
The annual development and seasonal distribution of predominant viruses were also analyzed, showing that Rotavirus was the most frequent during the period 2008-2010 (Fig. 2A), followed by a significant reduction (p = 0.043). Consideration of the frequency of Rotavirus as a function of the season (Fig. 2B) showed that the number of cases during the winter was significantly higher than in the other seasons (p = 0.016), which was not the case for the other viruses, especially Adenovirus, which showed no significant seasonal differences. There were peaks of higher relative frequency of viral diarrheas in April 2008 and May-July 2009, i.e., outside the winter period, although comparison of these frequencies with those observed for the same months in different years yielded no significant differences (p = 0.406).
With respect to parasites, the relative frequency was in general low, with no significant annual or seasonal differences throughout the study period, although a peak was observed in July 2008.
Discussion
In our study, Rotavirus, Campylobacter spp., and gastroenteric Salmonella were, in this order, the most frequently identified microorganisms in stool samples from patients with diarrhea. In general, bacterial and viral infections were more frequent in males than in females at all age ranges, in agreement with observations by other authors. In adult ages, this may be attributable to the higher frequency of risk practices in males than in females, including less care in the handling of food or the greater consumption of undercooked food (5). However, this would not explain the higher frequency among male children, because no sex differentiation in risk practices can be affirmed in early ages.
Various authors have reported that these three microorganisms show the highest incidence rates during infancy (6). We also found that the under-2-yr-old children had the highest frequency of viral diarrheas, especially due to Rotavirus (including frequent coinfections with Adenovirus), with bacterial infections being predominant at older ages. Among the latter, the mean age of pediatric patients with diarrhea caused by Campylobacter spp. was lower than the age of those with salmonellosis, as demonstrated in other studies (7), and this difference in age was also observed in the adult population.
Most of the stool samples that yielded positive results were of out-of-hospital origin, because the clinical procedure began in an outpatient setting. However, among the under-2-yr-old patients, the stool samples were mainly from hospital departments, either because, despite the out-of-hospital onset, they required hospital admission, a common practice due to their young age and to the clinical characteristics of diarrhea, which can course with intense dehydration (8-10), or because the viral diarrhea was nosocomial, which is also frequent (11).
Regardless of the etiology, patients with viral diarrhea more often required hospitalization and their mean hospital stay was longer than that of patients with bacterial diarrhea. Among the latter, hospitalization was more frequent when diarrhea was produced by Salmonella spp. but the duration of hospital stay, if required, was longer when the cause was Campylobacter spp. As indicated by other authors, there is a characteristic dissociation between the high frequency of diarrhea due to Campylobacter spp. and the low need for hospitalization, contrasting with observations in the case of Salmonella spp. (12). The greater length of hospital stays by patients with diarrhea due to G. lamblia is because the admission was intercurrent in 75 % of these cases.
The present study also showed a significant increase in diarrheas caused by Campylobacter spp. and a significant decrease in those due to Rotavirus during the last two years of the study, with no change in diarrheas caused by Salmonella spp. No studies have been published in our health area that could indicate whether this a current trend; however, various studies conducted in other areas of Spain during the past two decades have demonstrated that there has been an epidemiologic change, from situations in which rates of infection due to Salmonella spp. were higher than those caused by Campylobacter spp. (13) to a completely opposite situation, with a progressive increase in the frequency of clinical cases produced by Campylobacter spp. (12,14,15). At any rate, this increase was observed during the last two years of the study and we could not establish whether it was due to epidemic outbreaks, because of the lack of recorded data to confirm this possibility with complete reliability; higher peaks of frequency of bacterial diarrheas were observed in May 2011, September 2011, and August 2012, which may correspond to outbreaks, but they were not documented as such. For this reason, cannot establish whether this trend will be maintained trend in subsequent years or is an exceptional situation that may subsequently be reversed.
On the other hand, two oral vaccines against Rotavirus formed by live attenuated viruses (one monovalent, which includes serotype G1P1A, and another pentavalent, with serotypes G1 to G4 and P1A) have been commercialized in Spain since 2007, and both have demonstrated their effectiveness in various studies (16-18). Although these vaccines have not yet been included in the vaccine calendar, they are recommended by various scientific societies, including the Spanish Pediatrics Association (Asociación Española de Pediatría), and are frequently prescribed and recommended to parents by pediatricians for infants under 6 months old. According to some authors, this has translated into a gradual increase in vaccine coverage year by year (19) and has been associated with a significant reduction in the incidence of diarrheas by Rotavirus and especially in hospitalizations for this reason (8,19). However, some authors consider that it is difficult to determine the true data on vaccine coverage in our country, and it is therefore not possible to establish a definitive causal relationship (10).
The pattern of seasonal distribution of the most frequent infectious diarrheas in this study was similar to that reported by other authors: Salmonella spp. was detected more frequently during the summer and autumn (13,20), Campylobacter spp. during the spring (5), and Rotavirus during the winter (8,19). Although it is possible that the detected peaks may correspond to epidemic outbreaks, the recorded data do not allow this to be definitively confirmed.
Given that our study was retrospective and based on the reports emitted by the Microbiology Department, an important limitation is that these reports occasionally lacked some important demographic data for the patients (because they are sometimes not included in the order form attached to the sample or, in the case of requests from Primary Care, because it was not possible to access the clinical records electronically). Therefore, these data were not complete for all study patients. It was only possible to gather data, although incomplete, on data such as the sex and age of patients, the community or hospital origin of the sample, and the department ordering the microbiological study. Likewise, the systematic gathering of some important clinical data related to the clinical process in each of the study episodes was not possible (including personal history of interest, characteristics of the stool, pathological products, or presence of abdominal pain, fever, dehydration, neurological disorders, biochemical and/or hematological analytical disorders, etc.). This was because in most cases the medical reports and clinical records did not include this information, the report was incomplete in cases in which some data could be gathered, or it was not possible to differentiate whether clinical/analytical data in the report were due to the clinical process that originated the request for the microbiological and/or parasitological analysis or to other concomitant diseases. Thus, in the cases in which the same microorganism was detected in two or more samples obtained with an interval of > 1 week, it could not be determined whether this situation was due to a persistence of the microorganism in the patient or to a re-infection by the same microorganism, because there was no negative study between the two samples and there were no data indicating the clinical evolution of the patient during this time.
Another important limitation is that, as in other studies, patients with symptoms of diarrhea and/or non-acute abdominal pain whose physicians did not order stool microbiological and/or parasitological study were not recorded; hence, the true data are underestimated and largely determined by the severity of the clinical process. Nevertheless, the data provided in the present study are comparable with those of various regional, national, and international studies conducted in similar situations.
In conclusion, there was a significant increase in the frequency of diarrheas due to Campylobacter spp. in our health area during the study period and a significant decrease in those produced by Rotavirus, while the frequency of processes caused by Salmonella spp. did not change. These microorganisms also showed a marked seasonal distribution. Further periodical studies in the same area are necessary to definitively confirm these trends and verify whether they truly correspond to an epidemiologic change or simply respond to exceptional situations.
References
1. Guerrant RL, Van Gilder T, Steiner TS, Thielman NM, Slutsker L, Tauxe RV, et al. Practice guidelines for the management of infectious diarrhea. Clin Infect Dis 2001;32:331-51. [ Links ]
2. Thielman NM, Guerrant RL. Clinical practice. Acute infectious diarrhea. N Engl J Med 2004;350:38-47. [ Links ]
3. Kolling G, Wu M, Guerrant RL. Enteric pathogens through life stages. Front Cell Infect Microbiol 2012;2:114. [ Links ]
4. De Wit MA, Hoogenboom-Verdegaal AM, Goosen ES, Sprenger MJ, Borgdorff MW. A population-based longitudinal study on the incidence and disease burden of gastroenteritis and Campylobacter and Salmonella infection in four regions of The Netherlands. Eur J Epidemiol 2000;16:713-8. [ Links ]
5. Luquero Alcalde FJ, Sánchez Padilla E, Eiros Bouza JM, Domínguez-Gil González M, Gobernado Serrano C, Bachiller Luquer R, et al. Trend and seasonal variations of Campylobacter gastroenteritis in Valladolid, Spain. A five-year series, 2000-2004. Rev Esp Salud Publica 2007;81:319-26. [ Links ]
6. Bellido-Blasco JB, González-Cano JM, Galiano-Arlandis JV, Herrero-Carot C, Tirado-Balaguer MD, Arnedo-Pena A, et al. Risk factors for the occurrence of sporadic Campylobacter, Salmonella and rotavirus diarrhea in preschool children. An Pediatr (Barc) 2007;66:367-74. [ Links ]
7. Fajó-Pascual M, Godoy García P, Aramburu Arnuelos J, Nogués Biau A. Risk factors for sporadic cases of Campylobacter infection in children. Gac Sanit 2009;23:326-9. [ Links ]
8. García-Basteiro AL, Bosch A, Sicuri E, Bayas JM, Trilla A, Hayes EB. Hospitalizations due to rotavirus gastroenteritis in Catalonia, Spain, 2003-2008. BMC Res Notes 2011;4:429. [ Links ]
9. Lopez-de-Andres A, Jimenez-Garcia R, Carrasco-Garrido P, Alvaro-Meca A, Galarza PG, de Miguel AG: Hospitalizations associated with rotavirus gastroenteritis in Spain, 2001-2005. BMC Public Health 2008;8:109. [ Links ]
10. Rivero MJ, Román E, García MI, Zafra M, Gil A, González-Escalada A. Epidemiology of community-acquired rotavirus gastroenteritis in Fuenlabrada (Madrid). Enferm Infecc Microbiol Clin 2011;29:432-4. [ Links ]
11. Gutiérrez-Gimeno MV, Martin-Moreno JM, Díez-Domingo J, Asensi-Botet F, Hernández-Marco R, Correcher-Medina P, et al. Nosocomial rotavirus gastroenteritis in Spain: A multicenter prospective study. Pediatr Infect Dis J 2010;29:23-7. [ Links ]
12. Bellido-Blasco JB, Celades-Porcar ME, Tirado-Balaguer MD, González-Cano JM, Gil-Ortuño M, Arnedo-Pena A. Infectious diarrhea study in Castellón, Spain (EDICS): Population incidence of sporadic cases in 2004 and comparison with the year 2000. Med Clin (Barc) 2006;127:448-50. [ Links ]
13. Pérez-Ciordia I, Rezusta A, Mairal P, Larrosa A, Herrera D, Martínez-Navarro F. Comparative study of Salmonella and Campylobacter infections in Huesca. 1996-1999. Rev Esp Salud Publica 2001;75:459-65. [ Links ]
14. Bellido JB, Galiano JV, Tirado MD, González-Cano JM, Safont L. Incidence of sporadic cases of the most frequent intestinal infections in Castellon. Rev Esp Salud Publica 2003;77:629-38. [ Links ]
15. Fajó-Pascual M, Godoy P, Ferrero-Cáncer M, Wymore K. Case-control study of risk factors for sporadic Campylobacter infections in northeastern Spain. Eur J Public Health 2010;20:443-8. [ Links ]
16. Castilla J, Beristain X, Martínez-Artola V, Navascués A, García Cenoz M, Alvarez N, et al. Effectiveness of rotavirus vaccines in preventing cases and hospitalizations due to rotavirus gastroenteritis in Navarre, Spain. Vaccine 2012;30:539-43. [ Links ]
17. Ruiz-Palacios GM, Pérez-Schael I, Velázquez FR, Abate H, Breuer T, Clemens SC, et al. Safety and efficacy of an attenuated vaccine against severe rotavirus gastroenteritis. N Engl J Med 2006;354:11-22. [ Links ]
18. Vesikari T, Matson DO, Dennehy P, Van Damme P, Santosham M, Rodriguez Z, et al. Safety and efficacy of a pentavalent human-bovine (WC3) reassortant rotavirus vaccine. N Engl J Med 2006;354:23-33. [ Links ]
19. Gil-Prieto R, Gonzalez-Escalada A, Alvaro-Meca A, Garcia-Garcia L, San-Martin M, González-López A, et al. Impact of non-routine rotavirus vaccination on hospitalizations for diarrhoea and rotavirus infections in Spain. Vaccine 2013;31:5000-4. [ Links ]
20. Pérez-Ciordia I, Ferrero M, Sánchez E, Abadías M, Martínez-Navarro F, Herrera D. Salmonella enteritis in Huesca. 1996-1999. Enferm Infecc Microbiol Clin 2002;20:16-21. [ Links ]
![]() Correspondence:
Correspondence:
Antonio Sorlózano Puerto
Department of Microbiology
Facultad de Medicina.
Universidad de Granada
Avda. Madrid, 11.
18012 Granada, Spain
e-mail: asp@ugr.es
Received: 23-08-2014
Accepted: 03-11-2014

