










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 n.3 Madrid Mar. 2015
PICTURES IN DIGESTIVE PATHOLOGY
Acute gastric volvulus: A case report
Vólvulo gástrico agudo. A propósito de un caso
María Pilar Guillén-Paredes and José Luis Pardo-García
General and Digestive Surgery Department. Hospital Comarcal del Noroeste. Caravaca de la Cruz, Murcia
Case report
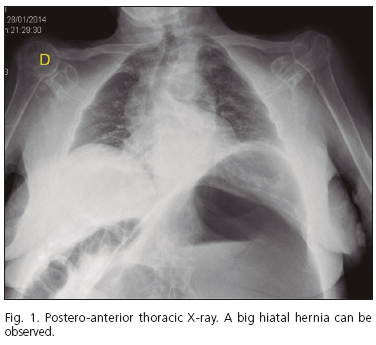
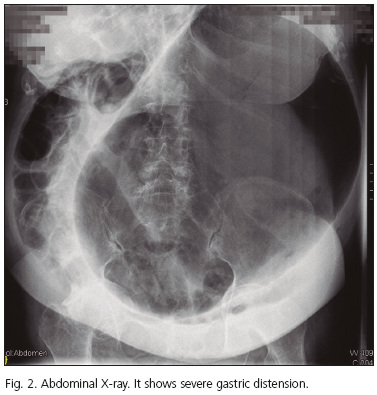
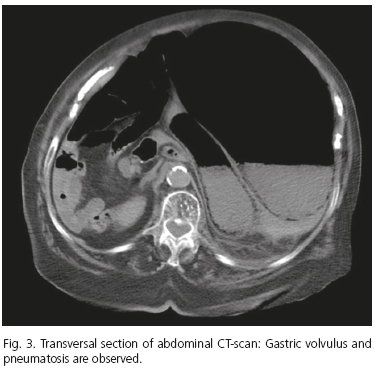
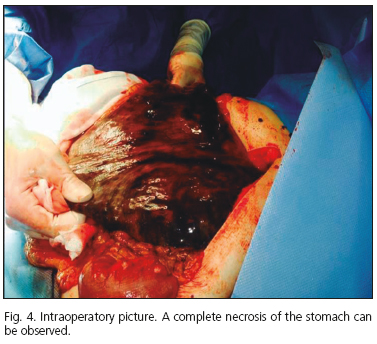
An 87-year-old female patient, with previous history of high blood pressure, came to the Emergency Department with complaints of intensive abdominal pain in the last 24 hours, associated with nausea without vomiting. Physical examination determined blood pressure: 120/60 mmHg, heart rate: 110/min, none diuresis, abdominal distension and epigastric pain without signs of peritonitis. Lab report: 12.900 leukocytes/µL (90 % neutrophils), creatinine level: 3 mg/dL, urea level: 90 mg/dL. A nasogastric tube was inserted and abundant gas was obtained through it. Thorax and abdomen radiography scan were made (Figs. 1 and 2). A CT-scan was also performed (Fig. 3). This patient underwent an emergency laparotomy and a complete gastric necrosis was found (Fig. 4). A total gastrectomy was initiated but the patient suffered an intraoperatory cardiac arrest. Finally, the patient died in spite of cardiopulmonary reanimation.
Discussion
Gastric volvulus (GV) is an uncommon disease which can be life threatening. Its incidence is unknown, due to a mild intermittent and chronic type of this disease. GV involves the rotation of more than 180o of the stomach in its organoaxial axis (59 %), in its mesenteroaxial axis (29 %), or both (2 %) (1). It causes ischemia of the stomach, and, if not recognized early, it can lead to gastric necrosis. It is important to note that necrosis of the stomach is infrequent, due to its rich blood supply, but when it appears, the mortality rate is approximately 30-50 % (2). The etiology is secondary to diaphragmatic defects in the 70 % of the cases, with paraesophageal hernia being the main cause (3). Classic symptoms of acute GV are known as Bochardt's triad (severe epigastric pain, nonproductive vomiting and inability to pass a nasogastric tube) (4) and they appear in 50 % of the cases (5). Diagnosis is usually done by CT-scan, although diagnostic signs will show up in a plain X-ray. Plain radiographic findings include an intrathoracic portion of the stomach, severe gastric distension and lack of air in the distal bowel. The main treatment is surgical and includes laparotomy, gastric detorsion, repair of associated diaphragmatic hernia and fixation or anterior gastrostomy. Gastrectomy is indicated in cases of gastric necrosis (5). The endoscopic approach alongside percutaneous gastrostomy is the treatment of choice for high risk patients without gastric necrosis (6).
References
1. Lesquereux-Martínez L, Macías-García F, Ferreiro R, Martínez-Castro J, Gamborino-Caramés E, Beiras-Torrado A. Acute gastric volvulus: A surgical emergency. Rev Esp Enferm Dig 2011;103:219-20. [ Links ]
2. Wijesuriya S, Watura R. Acute gastric volvulus: An uncommon complication of a hiatus hernia. BMJ Case Rep 2011. pii: bcr0920114753. doi: 10.1136/bcr.09.2011.4753. [ Links ]
3. González González JJ, Gómez Álvarez G, Álvarez Pérez JA, Navarrete Guijosa F, Trelles Martín A, Aza González J. Gastric volvulus. Presentation of a new case and review of the literature. Rev Esp Enferm Apar Dig 1989;75:59-62. [ Links ]
4. Borchardt M. Zur Pathologie und Therapie des Magen-Volvulus. Arch Klin Chir 1904;74:243-60. [ Links ]
5. Parker DM, Rambhajan A, Johanson K, Ibele A, Gabrielsen JD, Petrick AT. Urgent laparoscopic repair of acute symptomatic PEH is safe and effective. Surg Endosc 2013;27:4081-6. [ Links ]
6. Martínez-Garcia R, Peris-Tomas N, del Pozo CD, Vázquez-Targaron A, Martínez-Mas E, Trullenque Juan R, et al. Tratamiento del vólvulo gástrico agudo mediante abordaje laparoscópico. Cir Esp 2013;91:189-93. [ Links ]

