










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 no.4 Madrid abr. 2015
PICTURES IN DIGESTIVE PATHOLOGY
Hypercontractile "Jackhammer esophagus"
Esófago hipercontráctil Jackhammer
Javier García-Lledó, Ana Clemente-Sánchez, Beatriz Merino-Rodríguez, Óscar Nogales-Rincón, Cecilia González-Asanza and Pedro Menchén-Fernández-Pacheco
Gastroenterology Department. Hospital General Universitario Gregorio Marañón. Madrid, Spain
A 48-year-old woman with an ongoing history of dysphagia and chest pain during the last months was admitted to our hospital to perform manometry after ruling-out a cardiac origin of the symptoms.
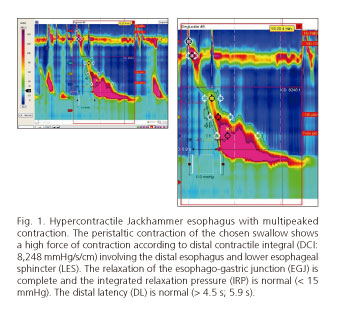
The patient provided an endoscopic report with no relevant findings. High resolution manometry was performed showing primary peristaltic esophageal contractions with elevated contractile pressures in each of the ten swallows studied, with a distal latency of 5.5 seconds and no disturbances in the relaxation of the lower esophageal sphincter (LES) with thus an integrated relaxation pressure (IRP) < 15 mmHg. One of the swallows showed, coincident with the chest pain (1), a multipeaked contraction with a distal contractile integral (DCI) greater than 8,000 mmHg/s/cm involving the distal esophagus and the LES, but not affecting the relaxation of the esophago-gastric junction (EGJ). A diagnosis of hypercontractile "Jackhammer esophagus" was established following the current Chicago classification of esophageal motility disorders (at least one swallow with DCI > 8,000 mmHg/s/cm) (2).
A hypercontractile esophagus is probably due to an excess of cholinergic activity, whilst type III achalasia and distal esophageal spasm are secondary to a loss of inhibitory neurons (3). These disorders are included in the differential diagnosis of non-cardiac causes of chest pain. Gastro-esophageal reflux is the most frequent cause related to hypermotility esophageal disorders; thus, proton pump inhibitors could provide some benefit to these patients. The management of hypercontractile esophagus is not validated (4). Medical approaches include the use of smooth muscle relaxants such as nitrates or calcium-channel blockers (nifedipine), phosphodiesterase-5 inhibitors (sildenafil) or even low-dose antidepressants, the latter could improve patient's reactions to pain without modifying the motility function. Other options include botulinum toxin injection, pneumatic dilation (5) in case of associated obstruction of the EGJ (not our case study) and POEM (peroral endoscopic myotomy).
Diagnosis is based on high resolution manometry, though an upper gastrointestinal endoscopy should precede this technique to discard organic causes of dysphagia and obstruction problems of the EGJ. Esophagram barium swallow study and pH-metry are supplementary diagnostic tests.
References
1. Conklin JL. Evaluation of esophageal motor function with high-resolution manometry. J Neurogastroenterol Motil 2013;19:281-94. [ Links ]
2. Bredenoord AJ, Fox M, Kahrilas PJ, et al. Chicago classification criteria of esophageal motility disorders defined in high resolution esophageal pressure topography (EPT). Neurogastroenterol Motil 2012;24(Supl.1):57-65. [ Links ]
3. Roman S, Pandolfino JE, Chen J, et al. Phenotypes and clinical context of hypercontractility in high resolution esophageal pressure topography (EPT). Am J Gastroenterol 2012;107:37-45. [ Links ]
4. Roman S, Kahrilas PJ. Management of spastic disorders of the esophagus. Gastroenterol Clin North Am 2013;42:27-43. [ Links ]
5. Pelletier AL, Pospai D, Merrouche M. Balloon against Jackhammer disorder. Case Rep Gastroenterol 2013;7(3):467-9. [ Links ]

