










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 n.6 Madrid Jun. 2015
LETTERS TO THE EDITOR
Gastric fundus splenosis mimicking stromal tumor
Key words: Splenosis. Gastric submucosal mass.
Dear Editor,
Splenosis is an infrequent acquired condition in which nodules of splenic tissue are transplanted in the peritoneal cavity due to splenic trauma or splenectomy (1). This letter to the editor describes the differential diagnosis of a gastric submucosal mass in a patient with background of splenectomy following abdominal trauma; the gastric mass was ultimately characterized as gastric splenosis.
Case report
A 53-year-old man was admitted to our hospital complaining of abdominal pain and early satiety for more than 2 years. There were no other special symptoms. He was carried out splenectomy 8 years ago because of traumatic rupture of spleen. The specific symptoms such as hematochezia, hematemesis, abdominal distension, dejecta turning small and anus distension were not occurred.
Physical examination showed no positive signs such as abdominal tension, tenderness or mass. Laboratory data show normal except neutrophil percentage 46.9%, eosinophils percentage 7.1% and blood total protein 55.9 g/L. Gastroscopy revealed a mass about 2.5x2.0 cm in size located at anterior wall of gastric greater curvature, with the surface mucosal hyperemia and swelling (Fig. 1 A and B). Endoscopic ultrasonography (EUS) revealed a slightly low echogenic mass which was about 2.2x1.5 cm in size originated from the muscularis propria. Local layers were not clear, and there were no enlarged lymph nodes imaging outside the wall (Fig. 1C). Mass was diagnosed as likely stromal tumor.
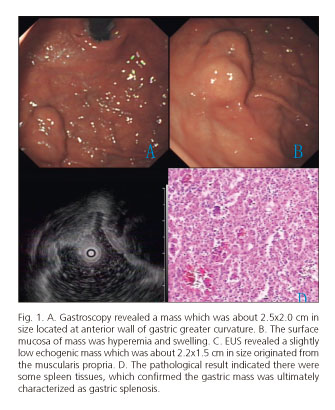
A 2.0x1.0x1.0 cm mass originated from the muscularis propria was found located at the anterior wall of gastric greater curvature, and surface was dark red, suspicious vascular tissue. The pathological result indicated there were some spleen tissues, which confirmed the gastric mass was ultimately characterized as gastric splenosis (Fig. 1D).
Discussion
Heterotopic splenosis that was reported for the first time by Von Kuttner in 1910 was the splenic autotransplants after trauma or other reasons splenectomy. Literature reported that the rate of splenosis was about 67% in the patient of splenic rupture and splenectomy (2). The exact pathogenesis is still not clear. However, there are some hypotheses such as potential cavity of the break, thrombosis of splenic vein, hematogenous dissemination of spleen tissues and so on. In this case, there was no stomach break, so we consider the possible thrombosis of splenic vein and hematogenous dissemination of spleen tissues. In fact, the splenosis can occur in many organs, such as the chest and abdomen. Most of the patients with no special symptoms do not require active intervention (3), except for few special position, size and shape of the mass (4).
Conventional gastroscopy can find the mass. However, the nature and origin of the lesion is always difficult to be determined. EUS plays an important role in differentiating the nature, origin and layer of the lesion. The current opinion is that when the splenosis is incidentally diagnosed in an asymptomatic patient, complete surgical removal is not indicated (5). In this case, the imaging of gastric fundus splenosis and stromal tumor were too similar to differentiate. All of the doctors who encounter a similar case like this should understand the patient medical history, check result and splenic autotransplants comprehensively. Nevertheless, the final diagnosis also needs the help of pathological examination.
Jing Bo Yang and De Liang Liu
Department of Gastroenterology. The Second Xiangya
Hospital of Central South University. Changsha, China
References
1. Carr NJ, Turk EP. The histological features of splenosis. Histopathology 1992;21:549-53. [ Links ]
2. Gruen DR, Gollub MJ. Intrahepatic splenosis mimicking hepatic adenoma. Am J Roentgenol 1997;168:725-6. [ Links ]
3. Kwok CM, Chen YT, Lin HT, et al. Portal vein entrance of splenic erythrocytic progenitor cells and local hypoxia of liver, two events cause intrahepatic splenosis. Med Hypotheses 2006;67:1330-2. [ Links ]
4. Marchant LK, Levine MS, Furth EE. Splenic implant in the jejunum: Radiographic and pathologic findings. Abdom Imaging 1995;20:518-20. [ Links ]
5. Ksiadzyna D, Peña AS. Abdominal splenosis. Rev Esp Enferm Dig 2011;103:421-6. [ Links ]

