










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 no.7 Madrid jul. 2015
PICTURES IN DIGESTIVE PATHOLOGY
Gastric metastasis originating from an adenocarcinoma of the endometrium
Metástasis gástrica de un adenocarcinoma de endometrio
Elvira Clavero-Fernández1, José Souto-Ruzo2, Pedro Alonso-Aguirre2, Rebeca Suárez-Fuentetaja1 and Mónica Álvarez-Martínez3
1General Internal Medicine Unit, 2Digestive Disease, and 3Pathology Departments. Complejo Hospitalario Universitario de A Coruña. A Coruña, Spain
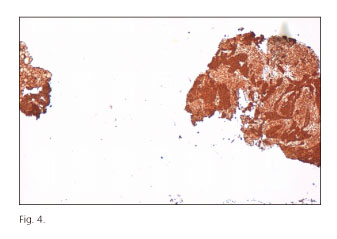
Endometrial cancer is the second most frequent gynaecologic tumour in Spain after breast cancer (1). For the majority of patients, the overall prognosis is positive because the cancer is diagnosed at an early stage. It most commonly spreads through lymphatic propagation and spreading via the bloodstream (commonly found in patients with abdominopelvic recurrences and in metastases from other organs) occurs in some advanced cases. Both local relapse and metastases often arise in the early years after treatment (2). Generally speaking, gastric metastases are infrequent while breast, broncho-pulmonary and melanoma primary tumours are the most common (3). We report the case of a 62-year-old woman that was diagnosed with a poorly-differentiated endometrial adenocarcinoma in 2009 and treated with total hysterectomy and bilateral adnexectomy, followed by radiation therapy and brachytherapy. In the follow-up, a necrotic tumour lesion was discovered during a routine CT scan in 2013. The tumour reached and entered the gastric fundus, gastric body, the upper part of the spleen and the tail of the pancreas; but there was no evidence of relapse in the pelvic region (Fig. 1). The patient suffered from postprandial epigastric pain, occasional melena and general malaise. Her general condition was good and the abdominal exploration was normal. The blood test revealed hypochromic microcytic anaemia. The upper gastrointestinal endoscopy showed a large gastric neoplasm (Fig. 2). Several biopsies were taken and histology was compatible with endometrial origin (Fig. 3). It is very unusual to see metastases originating from an adenocarcinoma of the endometrium, and gastric metastasis is even rarer. Nevertheless, taking into account the location and the oncological history, an immunohistochemistry test (CK7+, CK20-, vimentin+) was requested and the diagnosis was confirmed (Fig. 4). Other unusual facts included the absence of metastasis in other areas and the years passed since the diagnosis of the primary tumour. No published case has been found in the research carried out across PubMed.



References
1. Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin 2011;61:69-90. [ Links ]
2. Baños Madrid R, Martínez Crespo JJ, Morán Sánchez S, et al. Gastric metastasis from lung carcinoma. An Med Interna 2001;18:656-7. [ Links ]
3. Shumsky AG, Brasher PM, Stuart GC, et al. Risk-specific follow-up for endometrial carcinoma patients. Gynecol Oncol 1997;65:379-82. [ Links ]

