










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 no.7 Madrid jul. 2015
LETTERS TO THE EDITOR
Emphysematous gastritis associated with portal venous gas: Medical management to an infrequent acute abdominal pain
Gastritis enfisematosa con gas venoso portal: tratamiento conservador en abdomen agudo de causa infrecuente
Key words: Emphysematous gastritis. Medical management. Portal venous gas.
Palabras clave: Gastritis enfisematosa. Tratamiento conservador. Gas venoso portal.
Dear Editor,
Emphysematous gastritis is an infrequent cause of acute abdominal pain. Mortality ranges between 60-80%, requiring early diagnosis and intensive medical treatment to reduce morbidity and mortality.
Case report
An 85-year-old male with a past medical history of hypertension, cardiomyopathy hypertensive, chronic auricular fibrillation, ischemic stroke without sequels, recurrent respiratory infections and aspiration pneumonia, presented to Emergency Department with hip fracture after accidental fall. He was operated 3 days after correcting the coagulation index. The day after, the patient presented respiratory difficulty and low level of consciousness, due to pneumonia and he was treated with antibiotics. After 3 days, it was evident respiratory improvement, but he presented acute abdominal pain, associated with bloating and vomiting.
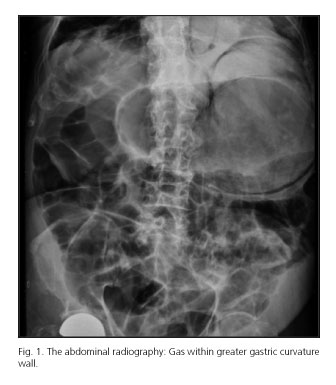
The abdominal radiography showed gas within greater gastric curvature wall (Fig. 1). The computed tomography scan showed diffuse and circumferential air within gastric wall extended to low esophagus, small amount of pneumoperitoneum adjacent to lesser gastric curvature, portal venous air and pneumomediastinum adjacent to low esophagus, suggesting emphysematous gastritis (Fig. 2).

The patient was treated with broad spectrum intravenous antibiotic, parenteral nutrition, inhibitors of proton pump and nasogastric tube. Ischemic etiology was ruled out when there was not evident arterial filling defects in computed angiotomography. After 11 days, a new computed tomography scan showed absence of esophageal and gastric pneumatosis (Fig. 2) and complete collapse of left lung. It was made a therapeutic bronchoscopy to remove secretions and mucous plugs. Restoration of airway patency and lung expansion was achieved. Antibiotic therapy was finished after 14 days and feeding was started successfully. After 96 hours, the patient showed respiratory difficulty and clinical worsening, causing his death.
Discussion
Air within the wall is a probable condition in abdominal organs, being less frequent in stomach (1). It is necessary a differential diagnosis between gastric emphysema and emphysematous gastritis (2), being completely different etiology, symptoms, prognosis and treatment. Gastric emphysema is caused by damage to the gastric mucosa; it is typically asymptomatic and resolves spontaneously. Emphysematous gastritis is caused by invasion of gas-producing bacteria through the stomach wall; it has a severe prognosis, high probability of complications and high mortality rate of 60% (1-5) (> 75% when associated to portal venous air) (3).
Gastric pneumatosis has different etiologies as mechanical (2,3,6), pulmonary (3), ischemic or infection causes [Escherichia coli, Enterobacter spp, Pseudomona aeruginosa, Clostridium perfringens (2-4), Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus, Clostridium welchii (1,7), Sarcina ventriculi (8), Mucormicosis (5) y Candida albicans (9)]. Infection is stimulated by several factors [diabetes (5), immunocompromise, renal failure, pulmonary pathology, neoplasm, pancreatitis (10), phytobezoar (5), major abdominal surgery (9), non-steroidal anti-inflammatory drug treatment or long term steroid use, alcohol abuse or caustic ingestion (1)].
Symptoms are frequently abdominal pain, nausea, vomiting or hematemesis, associated with fever, chills, tachycardia, tachypnea and toxic appearance (2,3).
The treatment is bowel rest and total parenteral nutrition, broad-spectrum antibiotic despite not isolating microorganisms (4); it may be associated antifungal therapy (5).
Surgical treatment is avoided in acute phase due to tissue friability (3), being necessary in septic status persistence or perforation (2,3), and in late strictures [present in 20% of cases (3,5)].
Our patient presented complete radiologic resolution after medical management, despite the presence of portal venous gas and its worst prognosis. The demise was probably due to an aspiration after oral feeding.
Carolina Guillén-Morales, Francisco Javier Jiménez-Miramón,
Teresa Carrascosa-Mirón and José María Jover-Navalón
Department of General and Gastrointestinal Surgery.
Hospital Universitario de Getafe. Getafe, Madrid. Spain
References
1. Muñoz C, Fernández R, Fonseca V, et al. Gastritis enfisematosa secundaria a ingesta de cáusticos: reporte de un caso. Gastroenterol Hepatol 2010;33:106-10. DOI: 10.1016/j.gastrohep.2009.09.007. [ Links ]
2. Szuchmacher M, Bedford T, Sukharamwala P, et al. Is surgical intervention avoidable in cases of emphysematous gastritis? A case presentation and literature review. Int J Surg Case Rep 2013;4:456-9. DOI: 10.1016/j.ijscr.2012.12.021. [ Links ]
3. Paul M, John S, Menon MC, et al. Successful medical management of emphysematous gastritis with concomitant portal venous air: A case report. J Med Case Rep 2010;4:140. DOI: 10.1186/1752-1947-4-140. [ Links ]
4. Gazquez I, Vicente de Vera P, Sheik Elard A, et al. Un caso de gastritis enfisematosa tratada con antibióticos con éxito. Ann Med Intern 2005;22:57-8. DOI: 10.4321/S0212-71992005000300018. [ Links ]
5. Iannuzzi J, Watson TJ, Litle VR. Emphysematous gastritis: A young diabetic's recovery. Int J Surg Case Rep 2012;3:125-7. DOI: 10.1016/j.ijscr.2011.12.002. [ Links ]
6. Khan SA, Boko E, Khookhar HA, et al. Acute gastric dilatation resulting in gastric emphysema following postpartum hemorrhage. Case Rep Surg 2012;2012:230629. [ Links ]
7. Nair R, Agrawal S, Nayal B. spontaneous resolution of emphysematous gastritis with vaso-occlusive disease- A case report. Malays J Med Sci 2013;20:68-70. [ Links ]
8. Laass MW, Pargac N, Fischer R, et al. Emphysematous gastritis caused by sarcina ventriculi. Gastrointest Endosc 2010;72:1101-3. DOI: 10.1016/j.gie.2010.02.021. [ Links ]
9. Loi TH, See JY, Diddapur RK, et al. Emphysematous gastritis: A case report and a review of literature. Ann Acad Med Singapore 2007;36:72-3. [ Links ]
10. Bloodworth LL, Stevens PE, Bury RF, et al. Emphysematous gastritis after acute pancreatitis. Gut 1987;28:900-2. DOI: 10.1136/gut.28.7.900. [ Links ]

