










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 no.10 Madrid oct. 2015
PICTURES IN DIGESTIVE PATHOLOGY
Direct peroral cholangioscopy with a conventional videogastroscope in a transplanted patient with anastomotic stricture and choledocholithiasis
Eduardo Rodrigues-Pinto, Pedro Pereira, Susana Lopes and Guilherme Macedo
Gastroenterology Department. Centro Hospitalar São João. Porto, Portugal
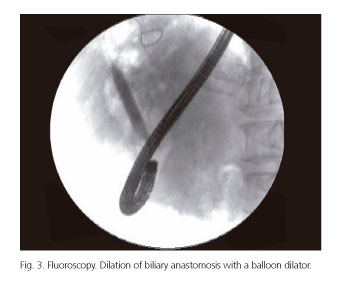
Female patient, 74 years-old, liver transplanted in 1991 due to primary biliary cirrhosis, later submitted to endoscopic retrograde cholangiopancreatography (ERCP) in 2009 because of biliary anastomotic stricture and choledocholithiasis. Successful sphincterotomy and placement of two plastic stents 8.5 Fr 7 cm was achieved, which were left in place for 3 months. The subsequent ERCP in 2010 revealed a proximal bile duct dilatation, without lithiasis. The patient was maintained on surveillance. In 2014, the patient presented with cholangitis. Magnetic resonance imaging revealed bile duct dilatation (24 mm) above the anastomosis, with upstream lithiasis. ERCP revealed a deformed duodenal papilla by previous sphincterotomy. Cholangiogram showed a dilated proximal bile duct (25 mm) with stenosis of surgical anastomosis and multiple subtraction defects, consistent with biliary stones (Fig. 1). Balloon catheter passage failed to remove the largest stone, despite the use of multiple devices. Direct peroral cholangioscopy (POC) was performed with a videogastroscope (Olympus® GIF-Q180), with identification of a membranous ring correspondent to anastomosis (Fig. 2), which was dilated (Boston Scientific® CRE™ Wireguided Balloon Dilator) under direct and fluoroscopic control up to 10 mm, with no complications (Fig. 3). Subsequent fragmentation of biliary stone (Figs. 4 and 5) was achieved under mechanical lithotripsy (Olympus® BML-110 Mechanical Lithotriptor) with removal of multiple fragments with balloon catheter (Olympus® Single Use 3-Lumen Extraction Balloon V). Final cholangiogram revealed no subtraction defects, with proper drainage at the end of the procedure. The patient was placed on prophylactic antibiotherapy (ciprofloxacin), remaining asymptomatic until now. Biliary strictures are one of the most common adverse events after liver transplantation, occurring in as many as 40% of patients in the postoperative period (1). The optimal strategy for treating these strictures remains to be defined (2). Direct POC is a useful technique for the study and treatment of biliary diseases, providing high quality endoscopic imaging of the biliary tree and anastomotic strictures (3). Once it uses a conventional endoscope it has a large diameter-working channel for interventional procedures, including tissue sampling with larger biopsy forceps, to differentiate from malignant strictures. Therapeutic interventions with direct POC can be expanded, like intraductal lithotripsy and evaluation of residual stones after mechanical lithotripsy for retained common bile duct stones (4). Dilation was performed only at cholangioscopy once a better visualization of the stenosis was possible, allowing dilating with a larger balloon and removing the stone under direct visualization.




References
1. Kao D, Zepeda-Gomez S, Tandon P, et al. Managing the post-liver transplantation anastomotic biliary stricture: Multiple plastic versus metal stents: a systematic review. Gastrointest Endosc 2013;77:679-91. [ Links ]
2. Dumonceau JM, Tringali A, Blero D, et al. European Society of Gastrointestinal Endoscopy. Biliary stenting: indications, choice of stents and results: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline. Endoscopy 2012;44:277-98. [ Links ]
3. Omuta S, Maetani I, Ukita T, et al. Direct peroral cholangioscopy using an ultraslim upper endoscope for biliary lesions. Hepatobiliary Pancreat Dis Int 2014;13:60-4. [ Links ]
4. Weigt J, Kandulski A, Malfertheiner P. Direct peroral cholangioscopy using ultraslim gastroscopes: High technical performance with important diagnostic yield. Gastrointest Endosc 2014;79:173-7. [ Links ]

