










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 no.10 Madrid oct. 2015
LETTERS TO THE EDITOR
Duodenal involvement by seminomatous tumors
Key words: Germ cell tumor. Seminoma. Gastrointestinal metastasis.
Dear Editor,
Testicular germ cell tumors (GCT), though rare (1%), represent the most common neoplasm among young men (1). Involvement of gastrointestinal (GI) tract in patients presenting such malignancies is due to three patterns: Infiltration from affected retroperitoneal lymph nodes or, less frequently, by peritoneal seeding and direct hematogenous metastatic spread (2,3). Its usual symptoms are bowel obstruction and digestive bleeding (2,3). However, GI infiltration from GCT is uncommon, ranging from 3.6% (1) to 5.1% (3). The article by Fu (4), published in 2012, identified only 15 cases.
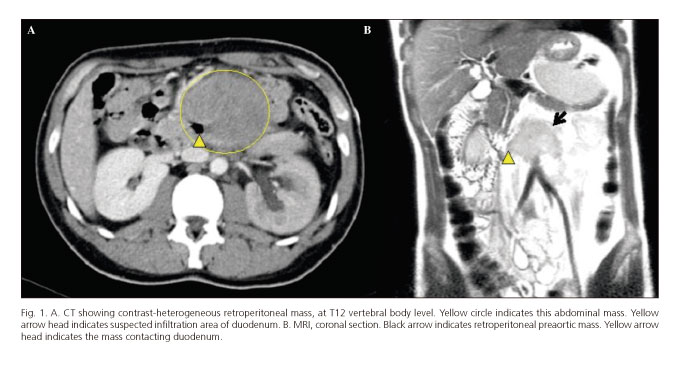
A 30-year-old male patient with a history of mental retardation presented with a 4-week general syndrome, vomiting and black stools, as reported by relatives. Physical examination: 120 beats per minute without hypotension, temperature 37.7 oC, cutaneous paleness and a big pulsatile painless mass occupying left hemiabdomen without rigidity. Patient refused rectal examination. Laboratory study: Hemoglobin 5.3 g/dl, without abnormalities in leukocytes, platelets and coagulation study, normal creatinine and mild hyponatremia and hypocloremia. Computer tomography (CT) showed contrast-heterogeneous retroperitoneal mass extending from celiac axis to common iliac arteries, which probably infiltrated the third duodenal portion (Fig. 1A).
After fluid resuscitation and transfusion, emergency gastroscopy revealed a partial duodenal stenosis with malignant aspect without current active bleeding. Biopsy was not performed because of suspected vascular component of the mass. Magnetic resonance imaging (MRI) reported giant bulky retroperitoneal lymph nodes as a possible origin (Fig. 1B). Finally, percutaneous CT-guided biopsy was performed, suggesting metastasis of seminoma. Testicular ultrasonography revealed a neoplasm in right testicle and the patient underwent inguinal radical orchiectomy (histopathology reported as pure seminoma, pT3), followed by chemotherapy (etoposide plus cysplatin). Twelve months after surgery, our patient is alive without any more gastrointestinal bleeding episodes. New CT demonstrated a 1.5 cm residual retroperitoneal mass.
Involvement of GI tract from advanced GCT is rare and so it is a duodenal location, as our patient presented, though its real frequency is not well defined. A postmortem study by Johnson (2) including 78 patients, observed 2 cases of duodenal metastasis out of 21 cases with GI metastasis from GCT. A series by Chait (3) analyzing 487 patients, reported 7 cases over 25, and Sweetenham (1) presented 3 cases out of 6, in 166 patients with GCT. From 1984 to 1989, Nord (5) registered 3 cases of duodenal metastasis over 5 patients with GI involvement from GCT. Finally, a radiological series by Husband (6) found no involvement of duodenum out of 650 patients with GCT, only one patient presented a GI metastasis located in the stomach.
In relation to the affinity for GI tract among different histological types of GCT, it is well-known that seminoma, the one diagnosed in our patient, has a lower GI metastasis rate than non-seminomatous tumors (1-3,5). Because of that, there are actually few cases in literature reporting involvement of duodenum due to metastatic seminoma (7,8). We have also identified two similar cases, both of which corresponded, however, to metastatic choriocarcinomas (9,10).
We conclude that severe anemia due to gastrointestinal bleeding in the context of retroperitoneal bulky metastatic mass infiltrating duodenum as first manifestation of pT3 pure seminoma is an extremely rare case, and this condition must be suspected when a young male patient refers such a clinical condition.
Acknowledgments
Authors thank Dr. A. Vargas and Dr. P. Díez (Gastroenterology and Endoscopy Department) and Dr. A. González and Dr. L. Fernández (Intensive Care Unit) for their contribution to the initial management of this patient. We are also thankful to all members of Radiology Department as well as Dr. E. Pérez (Pathology Department) for their help with imaging and histological diagnosis, and to Dr. V. Rodríguez Tesedo (Urology Department) and Dr. J. Puertas (Oncology Department) for patient's treatment and follow-up. Finally, we also thank Ms. M.L. de Andrés, our hospital librarian, for providing such a sheer number of articles required for our review.
Disclosures
The authors declare that they have no conflict of interest. The clinical case included in this article was presented as a poster during the XIX Spanish National Surgical Meeting, which took place in Burgos (Spain) from 23rd till 25th October 2013.
Mario Rodriguez-Lopez, Rosalía Velasco, Sara Mambrilla, Martin Bailon,
Katherine T. Plua, Luis M. Diez, José I. Blanco, Enrique Asensio,
Marta Gonzalo, Baltasar Pérez-Saborido and José L. Marcos
General and Digestive Surgery Department.
Hospital Universitario Río Hortega. Valladolid, Spain
References
1. Sweetenham JW, Whitehouse JM, Williams CJ, et al. Involvement of the gastrointestinal tract by metastases from germ cell tumors of the testis. Cancer 1988;61:2566-70. DOI: 10.1002/1097-0142 (19880615)61:12<2566::AID-CNCR2820611230> 3.0.CO;2-D. [ Links ]
2. Johnson DE, Appelt G, Samuels ML, et al. Metastates from testicular carcinoma: Study of 78 autopsied cases. Urology 1976;8:234-9. DOI: 10.1016/0090-4295(76)90374-5. [ Links ]
3. Chait MM, Kurtz RC, Hajdu SI. Gastrointestinal tract metastasis in patients with germ cell tumor of the testis. Am J Dig Dis 1978;23:925-8. DOI: 10.1007/BF01072468. [ Links ]
4. Fu S, Avezbakiyev B, Zhi W, et al. Germ cell cancer presenting as gastrointestinal bleeding and developing brain metastases: case report and review of the literature. Future Oncol 2012;8:1487-93. DOI: 10.2217/fon.12.133. [ Links ]
5. Nord C, Fosa SD, Giercksky KE. Gastrointestinal presentation of germ cell malignancy. Eur Urol 2000;38:721-4. DOI: 10.1159/000020368. [ Links ]
6. Husband JE, Bellamy EA. Unusual thoracoabdominal sites of metastasis in testicular tumors. Am J Roentgenol 1985;145:1165-71. DOI: 10.2214/ajr.145.6.1165. [ Links ]
7. Senadhi V, Dutta S. Testicular seminoma metastasis to the gastrointestinal tract and the necessity of surgery. J Gastrointest Cancer 2012;43:499-501. DOI: 10.1007/s12029-011-9274-0. [ Links ]
8. Miocinovic R, Abaza R. Testicular seminoma presenting with duodenal perforation: A case report. J Med Case Rep 2008;2:294. DOI: 10.1186/ 1752-1947-2-294. [ Links ]
9. Fosado Gayosso M, Pérez Hernández JL, Bernal Sahagun F, et al. Upper gastrointestinal bleeding as an initial manifestation of metastasis, secondary to a choriocarcinoma in a patient suffering from testicular mixed germ cell tumour. Rev Esp Enferm Dig 2011;103:46-7. DOI: 10.4321/S1130-01082011000100013. [ Links ]
10. Iglesias J, Lopez E, Macias F. Severe gastrointestinal bleeding secondary to duodenal metastasis from a choriocarcinoma. Rev Esp Enferm Dig 2009;101:720-2. DOI: 10.4321/S1130-01082009001 000008. [ Links ]

