










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 n.11 Madrid Nov. 2015
LETTERS TO THE EDITOR
Infarction of the greater omentum. Case report
Infarto de epiplón mayor. Caso clínico
Key words: Omentum. Omental torsion. Necrosis.
Palabras clave: Omento. Torsión. Necrosis.
Dear Editor,
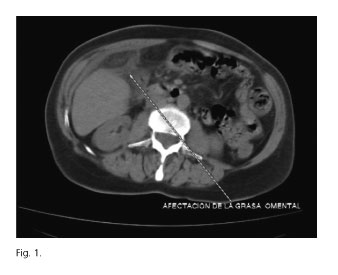
A 65-year-old female attended at Emergency Department complaining of abdominal pain in the upper right quadrant and a fever of 38 oC. Upon examination a painful mass of approximately 10 cm was detected below the right costal margin. Under analysis, leucocytosis and a slight left deviation was specified, with increased acute phase reactants. A right colon tumour was initially suspected. An X-ray was taken of the abdomen, with no findings, and a colonoscopy, which proved normal. In the computed tomography (CT), a thickening of fat was observed in the greater omentum with a mass effect, compatible with torsion of the greater omentum (Fig. 1). There were no alterations in other abdominal structures.
It was decided to provide conservative treatment with the fever disappearing and the symptoms reducing, with the patient being discharged on the seventh day. CT control was carried out 15 days after admission, with good clinical and radiological evolution. Three months later, the patient was asymptomatic and abdominal examination was normal.
Discussion
The infarction occurred due to its rotation on the transverse plane, which may cause vascular compromise with strangulation, necrosis and/or infarction. This occurs more frequently in paediatric age. There is no known aetiology. Predisposing factors include changes to omentum consistency, anatomical malformations or vascular abnormalities associated to triggers such as obesity or exercise. The secondary torsion is more frequent and it is associated to hernia injury, intra-abdominal inflammation, prior laparotomy or tumours, which give rise to a fixed point around which a segment of the omentum rotates.
The most frequent symptom is localised abdominal pain in the right hemiabdomen. For this reason, the differential diagnosis includes appendicitis, cholangitis, diverticulitis, etc. A mass is frequently associated to this area. Other symptoms and less specific signs are fever, nausea, vomiting, diarrhoea, or increased leukocyte count. The chosen technique for diagnosis is CT (1), which shows, as in this case, well-defined abdominal mass composed of interspersed fatty and fibrous folds, which are distributed concentrically or in a spiral, and the centre of which may contain a hyperdense vascular structure that descends perpendicularly to the transverse plane.
Surgical treatment was traditionally opted for, although good evolution has been observed in patients treated conservatively, especially in the case of segmentary infarctions (2) that do not present immediate complications. The CT (3) provides preoperative diagnosis in order to avoid emergency surgery and maintain an expectant attitude (4), and therefore act according to the patient's evolution, without considerable increase in complications being reported. There is a review of 43 cases in which conservative treatment is recommended, therefore preoperative image diagnosis is essential (4). However, some patients treated this way present complications such as sepsis or the formation of abscesses and adhesions. Surgical intervention must be considered where conservative treatment is not effective (5,6).
Rebeca Amo-Alonso1, Jaime de-la-Peña-Cadenato2, Andrea Loza-Vargas1,
Fernando Santos-Santamarta1, Ramón Sánchez-Ocaña-Hernández1 and Juan José Arenal-Vera3
1Department of Gastroenterology. Hospital Universitario Río Hortega. Valladolid, Spain.
Departments of 2Diagnostic Radiology and 3General Surgery. Hospital Campo Grande. Valladolid, Spain
References
1. Marcos R, Fernández JM, Lozano O, et al. Complete torsion of the greater omentum as a cause of acute abdomen. Contribution of computerized axial tomography to preoperative diagnosis. Cir Esp 2002;72:362-4. [ Links ]
2. Fernández-Rey CL. Primary omental infarction as cause of non-surgical acute abdomen: Imaging diagnosis. Rev Esp Enferm Dig 2010;102:498-9. DOI: 10.4321/S1130-01082010000800007. [ Links ]
3. Naffaa LN, Shabb NS, Haddad MC. CT findings of omental torsion and infarction: Case report and review of the literature. Clin Imaging 2003;27:116-8 DOI: 10.1016/S0899-7071(02)00524-7. [ Links ]
4. Park TU, Oh JH, Chang IT, et al. Omental infarction: Case series and review of the literature. J Emerg Med 2012;42:149-54. DOI: 10.1016/j.jemermed.2008.07.023. [ Links ]
5. Hirano Y, Oyama K, Nozawa H, et al. Left-sided omental torsion with inguinal hernia. World J Gastroenterol 2006;12:662-4. [ Links ]
6. Occhionorelli S, Zese M, Cappellari L, et al. Acute abdomen due to primary omental torsion and infarction. Case Rep Surg 2014;2014:208382. DOI: 10.1155/2014/208382. [ Links ]

