










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versão impressa ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 no.5 Madrid Mai. 2016
Acute hemorrhagic necrotizing pancreatitis in falciparum malaria
Pancreatitis aguda necroticohemorrágica en malaria falciparum
José Felipe Reoyo-Pascual, Carlos Cartón-Hernández, Xandra Valero-Cerrato, Raquel León-Miranda, Esther García-Plata-Polo, Rosa María Martínez-Castro, Miguel Ángel Álvarez-Rico and Francisco Javier Sánchez-Manuel
Service of General Surgery. Hospital Universitario de Burgos. Burgos, Spain
ABSTRACT
Malaria is a pathology caused by a parasite called Plasmodium, characteristic of tropical countries. The most frequent symptomatology includes cerebral malaria, jaundice, convulsive crisis, anemia, hypoglycemia, kidney failure and metabolic acidosis, among others. We are presenting the case of a patient diagnosed with malaria who suffered from acute hemorrhagic necrotizing pancreatitis and evolved poorly, as an example of this combination of symptoms, rarely found in our country.
Key words: Acute pancreatitis. Malaria. Falciparum.
RESUMEN
La malaria o paludismo es una patología causada por un parásito denominado Plasmodium, propia de países tropicales. Entre la sintomatología más frecuente destaca la malaria cerebral, ictericia, crisis convulsivas, anemia, hipoglucemia, fallo renal y acidosis metabólica, entre otras. Presentamos el caso de un paciente diagnosticado de paludismo, que presentó un cuadro de pancreatitis aguda necroticohemorrágica con mala evolución, como ejemplo inusual de dicha asociación descrita en nuestro país.
Palabras clave: Pancreatitis aguda. Malaria. Falciparum.
Introduction
Plasmodium falciparum malaria is uncommon in our country. It displays typical symptomatology based on high fever, kidney failure, hematological disturbance, etc. Pancreas affection in the clinical profile of falciparum malaria is an unusual combination, seldom found in Europe, which is the reason why we are presenting a case which may suggest its appearance.
Case Report
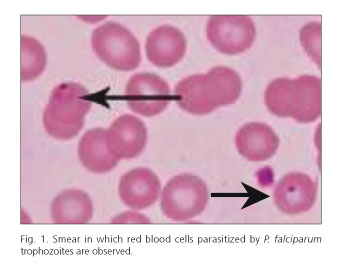
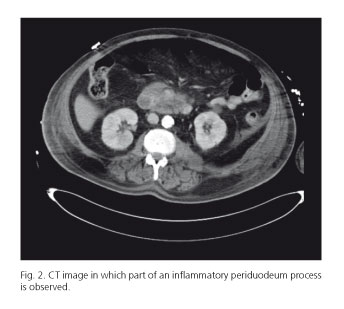
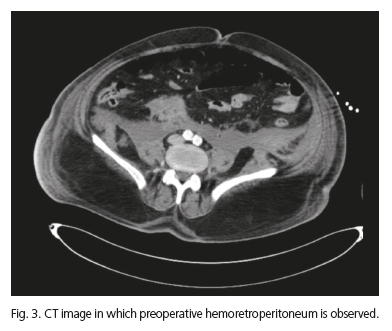
We are presenting the case of a 62-year-old male, a permanent resident of Angola, with a record of hypertension and hyperuricemia, who is admitted to our hospital with symptoms of fever and constitutional syndrome, which has been developing for one week. When the patient is examined, mucocutaneous jaundice is discovered, without any other pathology. During the analysis, leucocitosis is not observed, demonstrating a total of 6.7 mg/dl of bilirubin, 1.99 mg/dl of creatinine, 25 UI/l of amylase, 165 mg/dl procalcitonin. In the ultrasonography acalculous gallbladder disease with thin walls can be observed, without any other important discoveries. As he is diagnosed with sepsis accompanied by hematologic, hemodynamic and hepatic kidney failure, the patient is admitted to the Intensive Care Unit. Because it is suspected that he has malaria, a smear is carried out in this unit. As a result, some forms are objectified, which are compatible with Plasmodium falciparum (Fig. 1), with an index of > 21% parasitemia. Almost two weeks after the patient's admission to the Intensive Care Unit, he evolves poorly. For this reason, an upper digestive endoscopy is requested, in which one can observe a segmental area of the second part of the edematous duodenum, possibly related to the adjacent inflammatory process or the beginning of ischemia. With these findings and following clinical and analytical deterioration (intense leucocytosis, an increase in acute phase reactants, a discrete increase in amylase) confirming a clinical case of acute abdomen, abdominal CT is carried out, in which a suggestive image of a periduodenal inflammatory process can be observed, as well as hemoretroperitoneum data (Figs. 2 and 3). In the light of this data, and in the presence of the patient's unstable clinical condition, emergency surgery is required, in which duodenal pathology is not detected, revealing necrotizing hemorrhagic peripancreatic sphacelus, retroperinoteal hematoma, as well as globulose pancreas of hardened consistency accompanied by probable areas of steatonecrosis; proceeding to abdominal fluid drainage and admitting the patient to the Intensive Care Unit for observation. Discarding common causes of pancreatitis, such as lithiasis or toxin consumption, which are not found in this patient, and once medical literature is revised, a relation to malaria is suggested. Twenty-four hours after surgery is performed, the patient dies. Consequently, it is not possible to perform a necropsy.
Discussion
P. falciparum malaria is an extremely serious pathology, which involves a great variety of symptoms. The most important are coma, acidosis, anemia, DIC, shock and kidney failure, among others (1). Abdominal pain found in patients affected by malaria can generally be due to the following causes: Acalculous cholecystitis (2), splenic rupture (3), splenic infarction (4), splenic torsion (5), etc. The appearance of acute pancreatitis in patients suffering from malaria was first defined by Egdagl in 1907 (6), in the case of a series of 105 patients. In Asian and African countries, cases of pancreatitis in patients with malaria have been observed. Likewise, in 2007, Seshadri et al. (7) register and report a case of acute pancreatitis, revealing subdural hematoma in a patient suffering from falciparum malaria. Other authors such as Sharma et al., in 2012, register a case of acute pancreatitis in a patient with vivax malaria (8).
Referring to the physiopathological mechanism, authors such as Desai et al. (9) include pancreas ischemia caused by microvascular occlusion, possibly contributing to the presence of hemolytic anemia, which is characteristic of this pathology. For this reason, pancreatic vascular occlusion with the presence of parasitized erythrocytes caused by plasmodium has been discovered in several autopsies (10). In our case, the diagnosis of pancreatitis was intraoperative, in which it was not possible to confirm the findings with the necropsy; also, discarding other, more frequent causes such as alcohol consumption, cholelithiasis, dyslipidemia, hypercalcemia, toxins, etc. (11). According to what has been stated by authors such as Thapa et al. (12), in the clinical case of acute abdomen in patients suffering from plasmodium falciparum, the presence of acute pancreatitis is to be discarded. What we are especially concerned with in our case is not only the unusual relation between malaria and pancreatitis, but also the epidemiological anomaly which supposes the presence of malaria in our surroundings.
In conclusion, acute necrotizing hemorrhagic pancreatitis is a serious disease which must be considered in the case of acute abdomen symptoms found in patients suffering from malaria, after having discarded other, more frequent causes. Early diagnosis and providing early treatment will improve the survival odds of the patient.
References
1. Singh J, Dinkar A, Atam V, et al. An uncommon presentation of severe Falciparum Malaria: Acute pancreatitis. Int Res J Medical Sci 2014;2:26-8. [ Links ]
2. Anthoine-Milhomme MC, Chappuy H, Chéron G. Acute acalculous cholecystitis in a child returning from the Ivory Coast. Pediatr Emerg Care 2007;23:242-3, DOI: 10.1097/PEC.0b013e31803f5ab8. [ Links ]
3. Jiménez BC, Navarro M, Huerga H, et al. Spontaneus splenic rupture due to Plasmodium vivax in a traveler: Case report and review. J Travel Med. 2007;14:188-91. DOI: 10.1111/j.1708-8305.2007. 00112.x. [ Links ]
4. Kim A, Park YK, Lee JS, et al. A case of symptomatic splenic infarction in vivax malaria. Korean J Parasitol 2007;45:55-8. DOI: 10.3347/kjp.2007.45.1.55. [ Links ]
5. Cross AB. Diagnostic clue to acute splenic torsion in the tropics. Br Med J. 1974;3:564-6. DOI: 10.1136/bmj.3.5930.564. [ Links ]
6. Egdagl A. A review of 105 reported cases of acute pancreatitis, with special reference to a etiology with report of two cases. Johns Hopkins Med J 1907;18:130-2. [ Links ]
7. Seshadri P, Vimal A, Viggeswarpu S, et al. Acute pancreatitis and subdural haematoma in a patient with severe falciparum malaria: Case report and review of literature. Malar J 2008;7:97. DOI: 10.1186/1475-2875-7-97. [ Links ]
8. Sharma V, Sharma A, Aggarwal A, et al. Acute pancreatitis in a patient with vivax malaria. Journal of the Pancreas 2012;13:215-6. [ Links ]
9. Desai DC, Gupta T, Sirsat RA, et al. Malarial pancreatitis: Report of two cases and review of the literature. Am J Gastroenterol 2001;96:930-2. DOI: 10.1111/j.1572-0241.2001.03658.x. [ Links ]
10. Sarma PS, Kumar RS. Abdominal pain in a patient with falciparum malaria. Postfrad Med J 1998;74:425-7. DOI: 10.1136/pgmj.74.873.425. [ Links ]
11. Ghosh S, Kumar S, Sharma A. Unusual presentation of acute pancreatitis in falciparum malaria. Trop Prasitol 2014;4:56-57. DOI: 10.4103/2229-5070.129188. [ Links ]
12. Thapa R, Mallick D, Biswas B. Childhood Plasmodium falciparum malaria complicated by acute pancreatitis. Trop Doct 2010;40:184-5. DOI: 10.1258/td.2010.090420. [ Links ]
![]() Correspondence:
Correspondence:
José Felipe Reoyo Pascual.
Department of General Surgery.
Hospital Universitario de Burgos.
Avda. Islas Baleares, s/n.
09006 Burgos, Spain
e-mail: josefelipe82@hotmail.com
Received: 14-03-2015
Accepted: 15-04-2015
