










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 no.11 Madrid nov. 2016
PICTURES IN DIGESTIVE PATHOLOGY
Duodenal stump recurrence of gastric adenocarcinoma after subtotal gastrectomy
Armando Peixoto, João Santos-Antunes, Marco Silva and Guilherme Macedo
Department of Gastroenterology. Centro Hospitalar de São João. Faculty of Medicine. University of Porto. Porto, Portugal
Case Report
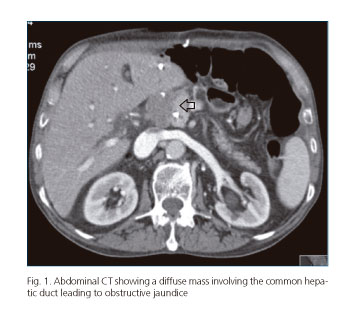
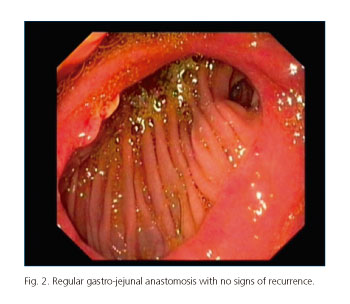
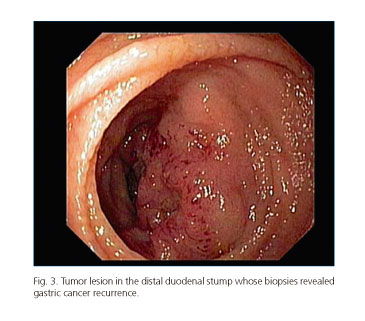
The authors present the case of a 71-year-old man with a history of a Billroth-II subtotal gastrectomy due to a mixed adenocarcinoma, stage pT4aN3aM0 (TNM classification), with adjuvant chemotherapy. Subsequent endoscopic and imaging evaluations revealed no signs of recurrence. Five years later, the patient was admitted with obstructive jaundice. Abdominal CT scan showed a diffuse mass close to the left hepatic lobe involving the common hepatic duct (Fig. 1), so a percutaneous biliary drainage was performed with symptomatic relief and analytical improvement. Consequent endoscopic evaluation integrity of the gastro-jejunal anastomosis (Fig. 2) and permeable efferent loop. In the duodenal stump, an obstructive mass distal to the papilla major was seen (Fig. 3). Biopsies confirmed it was a relapse of mixed gastric adenocarcinoma.
Discussion
Mixed type gastric cancers are highly metastatic and characterized by a more rapid disease progression, infiltrating both lymph nodes and the gastric wall, with a poorer prognosis than intestinal cancers (1). Locoregional recurrences after surgery seem to be more frequent in patients who have a fewer number of negative resected lymph nodes in the operative specimen (2). Duodenal stump late recurrences after curative surgery are rare, with less than six cases described in the literature, and usually present either as upper gastrointestinal bleeding or as an acute or chronic afferent loop syndrome with or without obstructive jaundice (3,4). One possible explanation results from invasion of the lymph nodes around the duodenal stump, which had been incompletely removed previously (5). Moreover, all previous cases involved the second, third or fourth portion of the duodenum, but none occurred in the first portion, making a metachronous cancer less probable. This case reinforces the need for a regular endoscopic follow-up of these patients, with careful exploration of the intestinal loops, particularly for more aggressive histological types.
References
1. Yashiro M, Chung YS, Nishimura S, et al. Establishment of two new scirrhous gastric cancer cell lines: Analysis of factors associated with disseminated metastasis. Br J Cancer 1995;72:1200. DOI: 10.1038/bjc.1995.486. [ Links ]
2. Li F, Zhang R, Liang H, et al. The pattern and risk factors of recurrence of proximal gastric cancer after curative resection. J Surg Oncol 2013;107:130. DOI: 10.1002/jso.23252. [ Links ]
3. Pouché A, Biasca F, Ottaviani GM, et al. Life-threatening digestive hemorrhage from duodenal recurrence of gastric cancer. Chir Ital 1999;51:405-8. [ Links ]
4. Yao NS, Wu CW, Tiu CM, et al. Percutaneous transhepatic duodenal drainage as an alternative approach in afferent loop obstruction with secondary obstructive jaundice in recurrent gastric cancer. Cardiovasc Intervent Radiol 1998;21:350-3. DOI: 10.1007/s002709900277. [ Links ]
5. Lee J, Lee K, Kim W. Duodenal stump cancer after Billroth-II distal gastrectomy for gastric cancer. Gastric Cancer 2009;12:118-22. DOI: 10.1007/s10120-009-0511-1. [ Links ]
