










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 n.12 Madrid Dec. 2016
PICTURES IN DIGESTIVE PATHOLOGY
A diffusely enlarged pancreas: the (un)usual suspect
Pedro Magalhães-Costa1, Maria José Brito2 and Pedro Pinto-Marques3
1Department of Gastroenterology. Hospital Egas Moniz. Lisbon, Portugal.
2Department of Pathology. Hospital Garcia de Orta. Lisbon, Portugal.
3Department of Gastroenterology. Hospital Garcia de Orta. Lisbon, Portugal
Case report
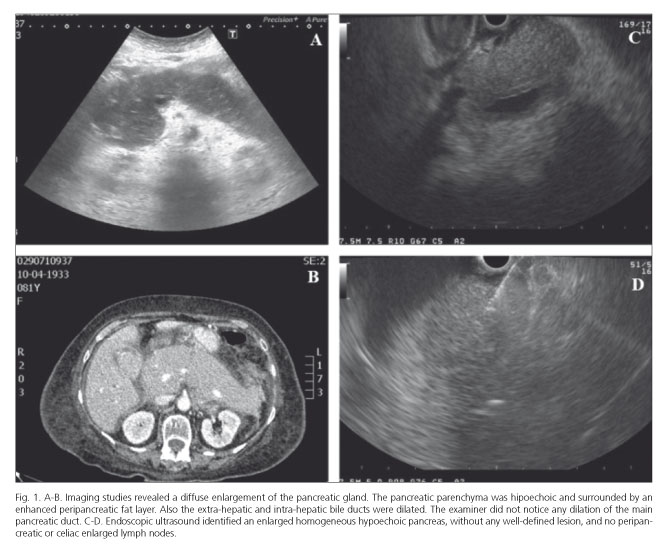
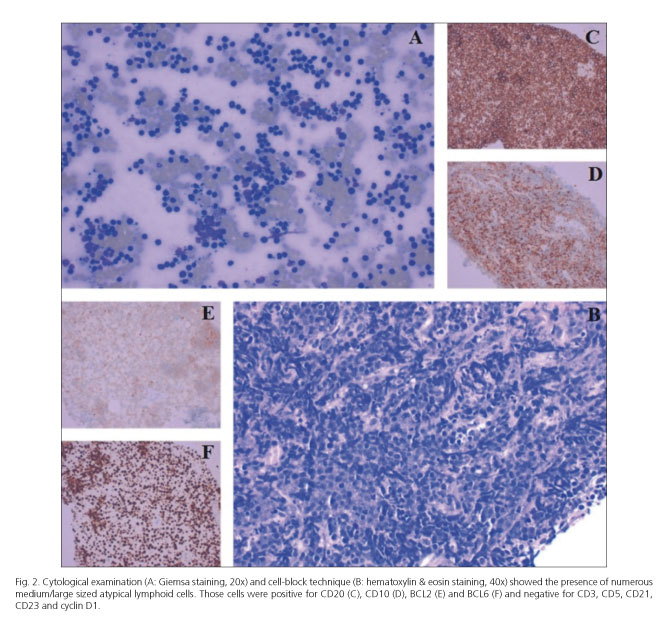
An 81-year-old female presented with obstructive jaundice and a non-specific clinical picture of nausea and appetite loss. Labs demonstrated a conjugated hyperbilirubinemia (7.7 mg/dL), increased aspartate aminotransferase and alanine aminotransferase (10x ULN and 8x ULN, respectively), increased lactate dehydrogenase (10x ULN) and serum lipase (3x ULN). CA 19.9 was 342 U/mL (ref. value < 37 U/mL). There was no evidence of peripheral lymphadenopathy or hepatosplenomegaly. Imaging (Fig. 1 A and B) revealed a marked homogeneous enlargement of the pancreas (without any well-defined mass), dilation of the extra and intra-hepatic bile ducts and ascites. Endoscopic ultrasound (Fig. 1 C and D) identified an enlarged homogeneous hypoechoic pancreas, without any well-defined lesion, no dilation of the main pancreatic duct, and no peripancreatic or celiac enlarged lymph nodes. A fine-needle biopsy was performed yielding, on cytological examination and cell-block technique (Fig. 2 A and B), numerous medium/large sized atypical lymphoid cells that displayed a B-cell lineage immunophenotype (Fig. 2 A-F). Even though further characterization (by flow cytometric immunophenotyping) could not be obtained, a final diagnosis of primary pancreatic lymphoma (PPL) was assumed.
Discussion
Primary pancreatic lymphoma is a remarkably rare tumor of the pancreas, representing approximately 0.5% of all pancreatic neoplasms and < 2% of all lymphomas (1,2). A correct diagnosis is crucial because therapeutic management differs from other pancreatic malignancies (pancreatic ductal adenocarcinoma, neuroendocrine tumor and metastases) (2,3). Two morphologic patterns of PPL are recognized: a focal form (occurring in the pancreatic head in 80% of cases) and a rarer diffuse/infiltrative pattern, as depicted herein, emulating an acute/autoimmune pancreatitis (1).
References
1. Battula N, Srinivasan P, Prachalias A, et al. Primary pancreatic lymphoma: Diagnostic and therapeutic dilemma. Pancreas 2006;33:192-4. DOI: 10.1097/01.mpa.0000227910.63579.15. [ Links ]
2. Du X, Zhao Y, Zhang T, et al. Primary pancreatic lymphoma: A clinical quandary of diagnosis and treatment. Pancreas 2011;40:30-6. DOI: 10.1097/MPA.0b013e3181e6e3e5. [ Links ]
3. Iglesias García J, Lariño Noia J, Domingues Muñoz JE. Endoscopic ultrasound in the diagnosis and staging of pancreatic cancer. Rev Esp Enferm Dig 2009;101:631-8. DOI: 10.4321/S1130-01082009000900006. [ Links ]
