










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.1 Madrid ene. 2017
https://dx.doi.org/10.17235/reed.2016.4190/2015
Risk factors for severity and recurrence of colonic diverticular bleeding
Natércia Joaquim1, Paulo Caldeira1,2, Artur Antunes2, Marta Eusébio2 and Horácio Guerreiro2
1Department of Biomedical Sciences and Medicine. Universidade do Algarve. Faro, Portugal.
2Department of Gastroenterology. Centro Hospitalar do Algarve. Faro, Portugal
ABSTRACT
Background: Colonic diverticular bleeding is the most common cause of lower gastrointestinal bleeding. Risk factors related to severity and repeated bleeding episodes are not completely clearly defined.
Objective: To characterize a Portuguese population hospitalized due to colonic diverticular bleeding and to identify the clinical predictors related to bleeding severity and rebleeding.
Methods: Retrospective analysis of all hospitalized patients diagnosed with colonic diverticular bleeding from January 2008 to December 2013 at our institution. The main outcomes evaluated were bleeding severity, defined as any transfusion support requirements and/or signs of hemodynamic shock, and 1-year recurrence rate.
Results: Seventy-four patients were included, with a mean age of 75.7 ± 9.5 years; the majority were male (62.2%). Thirty-six patients (48.6%) met the criteria for severe bleeding; four independent risk factors for severe diverticular bleeding were identified: low hemoglobin level at admission (≤ 11 g/dL; OR 18.8), older age (≥ 75 years; OR 4.7), bilateral diverticular location (OR 14.2) and chronic kidney disease (OR 5.6). The 1-year recurrence rate was 12.9%. We did not identify any independent risk factor for bleeding recurrence in this population.
Conclusion: In this series, nearly half of the patients hospitalized with diverticular bleeding presented with severe bleeding. Patients with low hemoglobin levels, older age, bilateral diverticular location and chronic kidney disease had a significantly increased risk for severe diverticular bleeding. In addition, a small number of patients rebled within the first year after the index episode, although we could not identify independent risk factors associated with the recurrence of diverticular bleeding.
Key words: Gastrointestinal bleeding. Colonic diverticulosis. Recurrence. Severity. Risk factors.
Introduction
Colonic diverticular bleeding (CDB) is the most common cause of lower gastrointestinal bleeding (LGIB), accounting for 30-50% of cases (1-4). In addition, bleeding is the second most common cause of complications in diverticulosis, after diverticulitis, and occurs in up to 15% of patients (5,6). Some of these patients will experience severe episodes requiring emergency medical assistance, hospitalization, and specific treatment, such as a blood transfusion and endoscopic or surgical treatments.
Several risk factors for CDB were identified in previous studies, namely previous episodes of CDB (7), right-sided diverticula (8,9), obesity (10), hypertension (11), diabetes mellitus, cardiovascular or cerebrovascular diseases (12). It has also been demonstrated that several medicaments are associated with an increased risk of CDB, including steroidal (13) and non-steroidal anti-inflammatory drugs (11,14,15) and antihypertensive medication (calcium-channel blockers) (13).
In order to better manage CDB in the clinical setting, major outcomes have been studied, namely mortality, severity and recurrence of bleeding. Mortality rates related to CDB are low, varying from 0 to 7% across studies (2,5,13,16,17). Severe bleeding is more difficult to assess, since its definition is not clearly established, and therefore different studies have used different criteria. Strate et al. (18) reported early predictors of severity in acute LGIB that were further used to develop a clinical prediction rule for a high-risk population (19). Lee et al. (20) performed the only study to date of risk factors predictive of severe diverticular hemorrhage, defined as systolic blood pressure below 90 mmHg, requirement for more than six units of transfusion or emergency surgery. These authors identified low initial hemoglobin levels, international normalized ratio (INR) > 1.5, decreased diastolic blood pressure, increased heart rate, and blood pressure medication as predictors of severe diverticular hemorrhage. Further studies are needed to consolidate these findings and clarify which patients would benefit from more aggressive interventions.
With regard to the recurrence of CDB, available data points to rates between 3.8 and 34.8%, within the first year (2,7,12,17,21-23). Although reports concerning the risk factors for rebleeding of colonic diverticula are scarce, older age, non-steroidal anti-inflammatory drugs, antiplatelet drugs, history of hypertension, peripheral vascular disease, renal deficiency, diverticulitis and shock at presentation have been associated with recurrence (12,23-26). However, results are inconsistent and additional studies are needed to better understand the factors implicated in repeated bleeding episodes.
The aim of this study was to characterize a Portuguese population hospitalized due to CDB and to identify the predictors related to severity and rebleeding.
Patients and methods
Patients
We conducted a retrospective cohort study that included all patients admitted and hospitalized at the Hospital de Faro, due to CDB, from January 2008 to December 2013. The study protocol was approved by the hospital ethics committee and was performed in accordance with the Declaration of Helsinki. CDB diagnosis was obtained based on clinical as well as colonoscopic criteria. All patients presented to the hospital Emergency Room with LGIB. After clinical examination, patients underwent an initial conservative treatment. Colonoscopy examination was performed when active bleeding was identified, in order to identify the bleeding site and source (5) as well as for therapeutic purposes. The timing of endoscopic procedures was determined by the need for urgent intervention, based on clinical criteria and, whenever possible, postponed until proper bowel cleaning preparation.
The diagnosis of CDB was made when the colonoscopy showed bleeding diverticula stigmata or when, in the presence of diverticulosis, no other probable source of bleeding was present. Patients with multiple possible bleeding sources, where active bleeding was not visualized on colonoscopy, were excluded from the study. This was the case for patients with colon cancer, inflammatory bowel disease, ulcers, angiodysplasia, and severe hemorrhoids. A total of 74 patients met these criteria and formed the study population. With regard to patients with more than one hospitalization related to CDB during the study period, we considered the first one as the index episode.
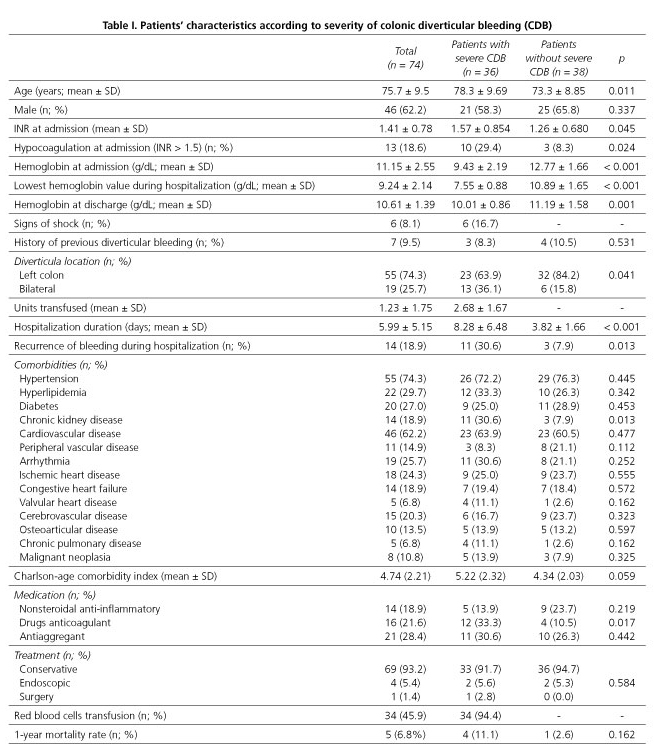
Data was collected from patient medical records. Demographic, clinical and treatment variables frequently related to LGIB prognosis in the literature were assessed (Table I).
Outcomes
The main clinical outcomes analyzed were CDB severity and 1-year recurrence rate. Additionally, mortality during hospitalization and 1-year mortality rate were also investigated.
In the absence of a reference standard for severe LGIB, we defined severe CDB based on the most reliable markers of severe bleeding, according to our clinical experience and relevant literature (18,20,22). Thus, patients with any red blood cell transfusion requirements and/or signs of hemodynamic shock (patients presenting with syncope, unconsciousness, light headedness, abnormal mental status, postural dizziness, or hypotensive and tachycardia) at admission or while hospitalized were grouped as "with severe bleeding".
Recurrent CDB was defined as rebleeding from colonic diverticula, diagnosed using the same methodology described above, leading to subsequent hospitalization, within a 12 month period from the index episode.
Data analysis
Demographic, clinical and treatment variables were compared between severe and non-severe bleeding groups and rebleeding and non-rebleeding patients. The associations between variables were tested using a Chi-squared or Fisher's exact analysis. The Mann-Whitney test was applied to compare quantitative variables between groups. Binary logistic regressions were applied to construct multivariable prediction models and to identify independent risk factors for severe bleeding and for recurrence of bleeding. Results are reported as odds ratios with 95% confidence intervals. Variables with a univariate significance of p < 0.10 were considered in this analysis. A p-value < 0.05 was considered as statistically significant.
Results
The study population consisted of 74 patients, of 75.7 ± 9.5 years of age, and 62.2% (n = 46) were males (Table I). At admission, hemoglobin levels were 11.15 ± 2.55 g/dL, 13 (18.6%) patients were hypocoagulated (INR > 1.5) and six (8.1%) presented signs of hemodynamic shock during the episode. Only seven (9.5%) patients had a past history of previous CDB. Colonoscopy examination revealed that 55 (74.3%) patients had diverticula in the left colon whereas 19 (25.7%) patients had diverticula in both the left and right colon. None of the patients presented diverticula exclusively in the right colon. The most prevalent co-morbidities in this population were hypertension, cardiovascular diseases, hyperlipidemia and diabetes.
Sixty-nine patients (93.2%) were treated conservatively and four underwent endoscopic treatment: two underwent endoscopic hemostatic clipping and the other two were given injection therapy with epinephrine or polidocanol (hydroxy-polyethoxy-dodecan). Both conservative and endoscopic treatments failed in only one patient, who underwent a sigmoidectomy. During hospitalization, 36 of the 74 patients required a blood transfusion, with mean requirements of 2.68 ± 1.67 units. None of the patients died during the index episode. Furthermore, only five (1-year mortality rate of 6.8%) patients died within one year after the index episode, all from causes not directly related to CDB.
Table I presents the relationship between patient characteristics and bleeding severity. Thirty-six (48.6%) patients met the criteria for severe bleeding. This group had a significantly higher mean age, higher proportion of bilateral diverticula, higher INR at admission, lower hemoglobin levels at admission and discharge, longer hospitalization, higher recurrence of bleeding during hospitalization, higher proportion of chronic kidney disease and anticoagulants use (p < 0.05). Although not statistically significant, patients with severe bleeding had a higher Charlson age comorbidity index (27) and higher 1-year mortality rate.
A multivariate model was tested including all possible predictors with a significant univariate association (p < 0.10) (Table II). The results identified four independent risk factors for severe CDB: low hemoglobin level at admission (OR 18.8), older age (OR 4.7), bilateral diverticular location (OR 14.2) and chronic kidney disease (CKD; OR 5.6).

Table III compares patients with and without bleeding recurrence within the first year after the index episode. For this analysis we included patients with at least one year follow-up. However, one of the patients who died during this period also experienced CDB recurrence and therefore was kept in the analysis. The incidence of recurrent bleeding at one year was 12.9% (n = 9), and 10.0% at six months. The median interval for recurrent bleeding was 94 days, varying from 8 to 320 days. No significant differences were found between the two groups except for the prevalence of congestive heart failure, which was higher in the patients with rebleeding (44.4% vs 16.4%; p = 0.048). The application of a binary logistic regression to construct a multivariable prediction model revealed that none of the variables were statistically significant. Therefore, we did not identify any independent risk factor for bleeding recurrence in this population.

Discussion
Diverticulosis of the colon is a common condition in industrialized countries, where it was considered to be the fifth most important gastrointestinal disease in terms of direct and indirect healthcare costs (28). Furthermore, the incidence of this disease has been growing in both Europe and the USA (29,30). Eighty per cent of individuals affected with diverticulosis are asymptomatic but up to 15% will develop CDB, which may be severe and also occur as repeated episodes.
The present study was developed to identify patients who are prone to severe CDB and rebleeding, in order to determine the adequate care of these patients. We identified 74 patients of advanced age, mainly males, who presented several co-morbidities and use of multiple medications. The dimension and characteristics of this group are similar to previous studies with similar designs and objectives (8,12,17,24-26). The high number of co-morbidities and subsequent medication is in accordance with patient age. As expected, diverticula were more prevalent in the left colon, which is in agreement with previous studies in western populations (9). In contrast, in Asian populations, diverticulosis is more common in the right colon and this difference has been associated with hereditary factors (31).
In our series, the majority of patients were managed conservatively. This is in accordance with previous studies that report that diverticular hemorrhage ceases spontaneously in about 90% of cases (32). Also the effective use of colonoscopy for hemostasis has been identified as a determinant factor for fewer operative interventions (3).
The mortality rate in the index episode was zero and only five patients died during the first year after the index episode, all from causes not directly related to CDB. Previous studies have also reported very low mortality rates associated with CDB (2,5,13,16,17). This indicates that mortality is not a major outcome of CDB and that the therapeutic measures applied to these patients are in fact effective.
In order to identify risk factors for severe bleeding, our first challenge was to define bleeding severity, since previous studies did not form a consensus with regard to the criteria to differentiate between patients with and without severe hemorrhage. In fact, Jensen et al. (5) defined severe bleeding as further hematochezia after colonoscopy, while Strate et al. (18) defined severe LGIB as the requirement of at least two units of packed red blood cells and/or a decrease in hematocrit of over 20%, and/or recurrent bleeding after 24 hours of clinical stability. Additionally, Lee et al. (20) also included transfusion support above six units of packed red blood cells into the bleeding severity definition. Furthermore, these authors used systolic blood pressure below 90 mmHg as a cut off for severe hemorrhage. In the present study, our option was to include in the severe bleeding group all the patients with any blood transfusion support and/or signs of hemodynamic shock at presentation. This decision was based on the fact that all of these patients required extra treatment measures, beyond the general conservative medical approach. Furthermore, the results show that this approach allowed us to distinguish between patients with worse outcomes, since this group had significantly lower hemoglobin levels at admission and discharge, longer hospitalization, higher recurrence of bleeding during hospitalization and higher mortality during the first year after the index episode, although this was not statistically significant.
In this series, 48.6% of patients had severe bleeding. Lee et al. (20) reported a severe bleed rate of 23% in a group of 99 patients hospitalized with diverticulosis in a Canadian study, while in the study of Strate et al. (18) severe LGIB occurred in 67% of the CDB patients subgroup. These differences could be explained by the different criteria used for severe bleeding. Thus, based on our criteria, one might expect that up to half of the patients presenting with CDB will suffer from a severe event.
Therefore, the identification of risk factors for bleeding severity is of great importance as it allows risk stratification and early medical intervention. In the present study we identified low hemoglobin at admission, older age, bilateral diverticular location and CKD as independent risk factors for severe CDB. Previously, Lee et al. (20) identified initial hemoglobin level as a predictor variable of severe CDB. In our series, this variable was the strongest predictor of severity. This was expected since transfusion needs, which is one of our criteria for severe bleeding, are determined mainly by low hemoglobin levels. Older age has been associated with the development of diverticulosis (6,9,33-36) and also with increased risk for LGIB (16) and CDB recurrence (26). As mentioned above, in the present study older age was also a predictive factor for severe CDB. This may be related to several hematological and/or vascular changes, typical of old age, which increase hemorrhagic tendency (37).
We also observed that patients with left and right colon diverticulosis in comparison with patients with diverticula located only in the left colon have a higher risk of severe bleeding. Yamada et al. (11), whilst studying risk factors for CDB, also reported that the proportion of bilateral diverticulosis was larger among patients with hemorrhage, and Faucheron et al. (9) and Suzuki et al. (8) stated that right-sided diverticula location was associated with a significant risk of bleeding, which was independent of age. Even though right-sided diverticula are less prevalent in the western population than left-sided ones (9), these results highlight the need to monitor patients with known right-sided diverticulosis closely and to alert clinicians to the greater risk of severe bleeding in these patients.
As previously mentioned, several co-morbidities were previously associated with increased risk of LGIB and, particularly, CDB. Despite the fact that the population we studied had several simultaneous co-morbidities, CKD was the only pathology predictive of severe hemorrhage. This is in accordance with the studies of Aytac et al. (26) and Nishikawa et al. (23), where renal insufficiency was associated with diverticular rebleeding. Kalman and Pedrosa (38), in their review of gastrointestinal bleeding in CKD patients, stated that this population has an increased risk of gastrointestinal bleeding and that its pathophysiology is often multifactorial. Even though there are no reports in the medical literature specifically linking gastrointestinal bleeding with uremic platelet dysfunction, this is thought to be the major factor that places chronic kidney patients at a higher risk of bleeding. Although these authors also point out that the incidence of lower gastrointestinal bleeding related to diverticulosis in the CKD population is not increased as compared to the general population, our study demonstrates that this condition increases the risk of severe CDB.
Although a hypocoagulated state at admission was not an independent factor predictive of severe CDB, INR was significantly higher in the severe bleeding group. In fact, the association between hypocoagulation and severe bleeding is intuitive, since it increases hemorrhagic tendency. Thus, whenever clinically possible, it is advisable to stop anticoagulant medication in patients with diverticulosis, especially for those patients with other risk factors for bleeding.
In the present study we also analyzed rebleeding rate. About 13% of the patients rebled within the first year after the index episode, which is in the range of the results from previous reports. This range is quite wide, varying from 3.8%, reported by Poncet et al. (17) in a French population, to 34.8%, presented by Nishikawa et al. (23) in a group of Japanese patients. This may be explained by the use of different criteria for recurrence, different follow-up periods and diverse intrinsic characteristics of the populations studied, such as the presence of risk factors for rebleeding (2,7,12,17,21-23). For instance, Okomoto et al. (12) argue that the high bleeding recurrence rate reported in their study may be explained by the high proportion of patients in their population with arteriosclerosis-related diseases and anti-coagulant or non-steroidal anti-inflammatory drugs use, which they found to be risk factors for diverticular rebleeding. In our study, the recurrence rate is relatively low, which may be explained by the fact that we only considered bleeding recurrence when it led to a new hospitalization, within 12 months from the index episode.
Even though previous studies addressed several risk factors for CDB recurrence (12,23-26), none of the factors we tested were predictive of a higher likelihood of rebleeding in our series, including bleeding severity in the index episode. Similar results were reported by Anthony et al. (39) for LGIB, where no risk factors for rebleeding were identified. The absence of independent predictive variables for colonic rebleeding may be related to the small sample size, although the studies mentioned above have similar size samples.
The only significant difference between the characteristics of the rebleeding and non-rebleeding group was in the prevalence of congestive heart failure, which was higher in the rebleeding patients. However, as mentioned, the rebleeding group is very small and further studies are needed to confirm the relationship between these variables.
A limitation of this study is its retrospective nature, as data was obtained from medical records. Therefore, this is dependent on their quality and there may be some errors in the data. In addition, this study was performed in a single center and the patient group was relatively small. This may have limited the identification of risk factors in this population. However, it is important to state that the dimension of this study population is similar to that of other studies with similar approaches (12,17,23-26).
In conclusion, nearly half of the patients hospitalized with CDB presented with severe bleeding, defined as transfusion support requirements and/or signs of hemodynamic shock. Patients with low hemoglobin levels at admission, older age, bilateral diverticular location and CKD showed a significantly increased risk of suffering severe CDB. Therefore, clinicians should pay special attention to these patients in clinical settings, namely by providing closer surveillance, earlier endoscopic examination and eventual endoscopic treatment. We also concluded that a small group of patients rebleed within the first year after the index episode. Further studies with a larger series are needed to identify independent risk factors associated with the recurrence of CDB.
References
1. Gostout CJ, Wang KK, Ahlquist DA, Clain JE, Hughes RW, Larson MV, et al. Acute gastrointestinal bleeding. Experience of a specialized management team. J Clin Gastroenterol 1992;14(3):260-7. DOI: 10.1097/00004836-199204000-00014. [ Links ]
2. Longstreth GF. Epidemiology and outcome of patients hospitalized with acute lower gastrointestinal hemorrhage: A population-based study. Am J Gastroenterol 1997;92(3):419-24. [ Links ]
3. Gayer C, Chino A, Lucas C, Tokioka S, Yamasaki T, Edelman DA, et al. Acute lower gastrointestinal bleeding in 1,112 patients admitted to an urban emergency medical center. Surgery 2009;146:600-7. DOI: 10.1016/j.surg.2009.06.055. [ Links ]
4. Lorenzo D, Nahon S. Diagnostic et prise en charge des hémorragies coliques diverticulaires. Acta Endosc 2013;43:166-74. DOI: 10.1007/s10190-013-0337-x. [ Links ]
5. Jensen DM, Machicado GA, Jutabha R, Kovacs TO. Urgent colonoscopy for the diagnosis and treatment of severe diverticular hemorrhage. N Engl J Med 2000;342:78-82. DOI: 10.1056/NEJM200001133420202. [ Links ]
6. Templeton AW, Strate LL. Updates in diverticular disease. Curr Gastroenterol Rep 2013;15(8):339. DOI: 10.1007/s11894-013-0339-z. [ Links ]
7. McGuire HH Jr. Bleeding colonic diverticula. A reappraisal of natural history and management. Ann Surg 1994;220(5):653-6. DOI: 10.1097/00000658-199411000-00008. [ Links ]
8. Suzuki K, Uchiyama S, Imajyo K, Tomeno W, Sakai E, Yamada E, et al. Risk factors for colonic diverticular hemorrhage: Japanese multicenter study. Digestion 2012;85:261-5. DOI: 10.1159/000336351. [ Links ]
9. Faucheron J, Roblin X, Bichard P, Heluwaert F. The prevalence of right-sided colonic diverticulosis and diverticular haemorrhage. Colorectal Dis 2013;15:e266-70. DOI:10.1111/codi.12137. [ Links ]
10. Strate LL, Liu YL, Aldoori WH, Syngal S, Giovannucci EL. Obesity increases the risks of diverticulitis and diverticular bleeding. Gastroenterology 2009;136(1):115-22. DOI: 10.1053/j.gastro.2008.09.025. [ Links ]
11. Yamada A, Sugimoto T, Kondo S, Ohta M, Watabe H, Maeda S, et al. Assessment of the risk factors for colonic diverticular hemorrhage. Dis Colon Rectum 2008;51:116-20. DOI: 10.1007/s10350-007-9137-8. [ Links ]
12. Okamoto T, Watabe H, Yamada A, Hirata Y, Yoshida H, Koike K. The association between arteriosclerosis related diseases and diverticular bleeding. Int J Colorectal Dis 2012;27:1161-6. DOI 10.1007/s00384-012-1491-x. [ Links ]
13. Jansen A, Harenberg S, Grenda U, Elsing C. Risk factors for colonic diverticular bleeding: A Westernized community based hospital study. World J Gastroenterol 2009;15:457-61. DOI:10.3748/wjg.15.457. [ Links ]
14. Aldoori WH, Giovannucci EL, Rimm EB, Wing AL, Willett WC. Use of acetaminophen and nonsteroidal anti-inflammatory drugs: A prospective study and the risk of symptomatic diverticular disease in men. Arch Fam Med 1998;7(3):255-60. DOI: 10.1001/archfami.7.3.255. [ Links ]
15. Strate LL, Liu YL, Huang ES, Giovannucci EL, Chan AT. Use of aspirin or nonsteroidal anti-inflammatory drugs increases risk for diverticulitis and diverticular bleeding. Gastroenterology 2011;140(5):1427-33. DOI: 10.1053/j.gastro.2011.02.004. [ Links ]
16. Peura DA, Lanza FL, Gostout CJ, Foutch PG. The American College of Gastroenterology Bleeding Registry: Preliminary findings. Am J Gastroenterol 1997;92(6):924-8. [ Links ]
17. Poncet G, Heluwaert F, Voirin D, Bonaz B, Faucheron JL. Natural history of acute colonic diverticular bleeding: A prospective study in 133 consecutive patients. Aliment Pharmacol Ther 2010;32:466-71. DOI: 10.1111/j.1365-2036.2010.04362.x. [ Links ]
18. Strate LL, Orav EJ, Syngal S. Early predictors of severity in acute lower intestinal tract bleeding. Arch Intern Med 2003;163(7):838-43. DOI: 10.1001/archinte.163.7.838. [ Links ]
19. Strate LL, Saltzman JR, Ookubo R, Mutinga ML, Syngal S. Validation of a clinical prediction rule for severe acute lower intestinal bleeding. Am J Gastroenterol 2005;100(8):1821-7. DOI: 10.1111/j.1572-0241.2005.41755.x. [ Links ]
20. Lee KK, Syed M, Shah SM, Moser MA. Risk factors predictive of severe diverticular haemorrhage. Int J Surg 2011;9(1):83-5. DOI: 10.1016/j.ijsu.2010.09.011. [ Links ]
21. Jensen DM, Singh B, Jensen ME, Sun N, Carrico M. How often do patients rebleed during long-term follow-up after an initial documented diverticular hemorrhage? Gastroenterology 2008;134(4 Suppl 1):A122-3. DOI: 10.1016/S0016-5085(08)60571-5. [ Links ]
22. Ríos Zambudio A, Montoya Tabares MJ, Rodríguez González JM, Febrero Sánchez B, Albaladejo Meroño A, Molina J, et al. Severe lower gastrointestinal tract bleeding due to diverticulosis. Gastroenterol Hepatol 2010;33(5):363-9. DOI: 10.1016/j.gastrohep.2010.02.003. [ Links ]
23. Nishikawa H, Maruo T, Tsumura T, Sekikawa A, Kanesaka T, Osaki Y. Risk factors associated with recurrent hemorrhage after the initial improvement of colonic diverticular bleeding. Acta Gastroenterol Belg 2013;76(1):20-4. [ Links ]
24. Niikura R, Nagata N, Yamada A, Akiyama J, Shimbo T, Uemura N. Recurrence of colonic diverticular bleeding and associated risk factors. Colorectal Dis 2011;14(3):302-5. DOI: 10.1111/j.1463-1318.2011.02611.x. [ Links ]
25. Fujino Y, Inoue Y, Onodera M, Kikuchi S, Endo S, Shozushima T, et al. Risk factors for early re-bleeding and associated hospitalization in patients with colonic diverticular bleeding. Colorectal Dis 2013;15(8):982-6. DOI: 10.1111/codi.12232. [ Links ]
26. Aytac E, Stocchi L, Gorgun E, Ozuner G. Risk of recurrence and long-term outcomes after colonic diverticular bleeding. Int J Colorectal Dis 2014;29(3):373-8. DOI: 10.1007/s00384-013-1804-8. [ Links ]
27. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol 1994;47(11):1245-51. DOI: 10.1016/0895-4356(94)90129-5. [ Links ]
28. Petruzziello L, Iacopini F, Bulajic M, Shah S, Costamagna G. Review article: Uncomplicated diverticular disease of the colon. Aliment Pharmacol Ther 2006;23:1379-91. DOI: 10.1111/j.1365-2036.2006.02896.x. [ Links ]
29. Masoomi H, Buchberg BS, Magno C, Mills SD, Stamos MJ. Trends in diverticulitis management in the United States from 2002 to 2007. Arch Surg 2011;146:400-6. DOI: 10.1001/archsurg.2010.276. [ Links ]
30. Jeyarajah S, Faiz O, Bottle A, Aylin P, Bjarnason I, Tekkis PP, et al. Diverticular disease hospital admissions are increasing, with poor outcomes in the elderly and emergency admissions. Aliment Pharmacol Ther 2009;30:1171-82. DOI: 10.1111/j.1365-2036.2009.04098.x. [ Links ]
31. Radhi JM, Ramsay JA, Boutros-Tadross O. Diverticular disease of the right colon. BMC Res Notes 2011;4:383-8. DOI: 10.1186/1756-0500-4-383. [ Links ]
32. Buttenschoen K, Buttenschoen DC, Odermath R, Beger HG. Diverticular disease-associated hemorrhage in the elderly. Langenbecks Arch Surg 2001;386(1):8-16. DOI 10.1007/s004230000198. [ Links ]
33. Schoetz DJ Jr. Diverticular disease of the colon: A century-old problem. Dis Colon Rectum 1999;42(6):703-9. DOI: 10.1007/BF02236921. [ Links ]
34. Jun SJ. Epidemiology of diverticular disease. Best Pract Res Clin Gastroenterol 2002;16(4):529-42. DOI: 10.1053/bega.2002.0328. [ Links ]
35. Afonso M, Pinto J, Veloso R, Freitas T, Carvalho J, Fraga J. Visceral fat: A key factor in diverticular disease of the colon. GE J Port Gastrenterol 2012;19(2):62-5. [ Links ]
36. Comparato G, Pilotto A, Franzè A, Franceschi M, DiMario F. Diverticular disease in the elderly. Dig Dis 2007;25:151-9. DOI: 10.1159/000099480. [ Links ]
37. Ranchini M. Hemostasis and aging. Crit Rev Oncol Hematol 2006;60:144-51. DOI: 10.1016/j.critrevonc.2006.06.004. [ Links ]
38. Kalman RS, Pedrosa MC. Evidence-based review of gastrointestinal bleeding in the chronic kidney disease patient. Semin Dial 2015;28(1):68-74. DOI: 10.1111/sdi.12301. [ Links ]
39. Anthony T, Penta P, Todd RD, Sarosi GA, Nwariaku F, Rege RV. Rebleeding and survival after acute lower gastrointestinal bleeding. Am J Surg 2004;188(5):485-90. DOI: 10.1016/j.amjsurg.2004.07.020. [ Links ]
![]() Correspondence:
Correspondence:
Natércia Joaquim.
Department of Biomedical Sciences and Medicine.
Universidade do Algarve.
Campus de Gambelas.
8005-139 Faro, Portugal
e-mail: naterciajoaquim72@gmail.com
Received: 18-01-2016
Accepted: 13-10-2016
