










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versão impressa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.4 Madrid Abr. 2017
PICTURES IN DIGESTIVE PATHOLOGY
Hepatocellular carcinoma presenting with Budd-Chiari syndrome, right atrial thrombus and pulmonary emboli
Luís Carvalho Lourenço, David Valadas Horta, Sara Folgado Alberto and Jorge Reis
Department of Gastroenterology. Hospital Professor Doutor Fernando Fonseca. Amadora, Portugal
Case report
A 47-year-old patient presented with a two-week history of right upper quadrant pain, abdominal distention and new onset of shortness of breath. He had a history of intravenous drug abuse, no alcohol consumption and denied any known liver disease. On physical examination, he was tachypneic and had dullness in the flanks.
His blood analysis at admission was as follows: hemoglobin, 12.9 g/dL; leukocyte count, 6,800/uL; platelet count, 63,000/uL; INR, 2.1; serum creatinine, 1.27 mg/dL; liver biochemistry tests were notable for marginal derangement, HBsAg was negative, anti-HCV was positive, HCV RNA was 367,498 IU/ml and alpha-fetoprotein was 992 mg/dL.
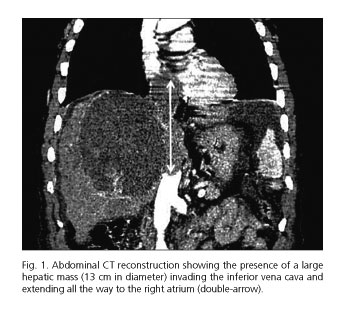
Abdominal ultrasound showed a right liver lobe mass (13 cm in diameter) with inferior vena cava (IVC) thrombosis and mild peri-hepatic ascites. A 2D echocardiogram showed a presumed right atrial tumor thrombus. A multiphasic contrast-enhanced abdominal tomography (CT) confirmed a hepatocellular carcinoma (HCC) with IVC obstruction and extensive tumoral thrombus to the right atrium (14 cm long) (Fig. 1). Chest CT also revealed bilateral pulmonary emboli, pleural effusions and pulmonary metastasis.
Given the advanced disease, he was discharged with best supportive care.
Discussion
Secondary Budd-Chiari syndrome (BCS) (1) is found in less than 1% of HCCs and is an extremely rare form of presentation (2,3). Here, we illustrate a rare case of HCC complicating chronic hepatitis C and presenting with secondary BCS, tumoral thrombus in the IVC extending into the right atrium and pulmonary embolism.
References
1. Horton JD, San Miguel FL, Membreno F, et al. Budd-Chiari syndrome: Illustrated review of current management. Liver Int 2008;28:455-66. DOI: 10.1111/j.1478-3231.2008.01684.x. [ Links ]
2. Boutachali S, Arrive L. Budd-Chiari syndrome secondary to hepatocelular carcinoma. Clin Res Hepatol Gastroenterol 2011;35:693-4. DOI: 10.1016/j.clinre.2011.07.006. [ Links ]
3. Kage M. Budd-Chiari syndrome and hepatocellular carcinoma. J Gastroenterol 2004;39:706-7. DOI: 10.1007/s00535-004-1393-y. [ Links ]
