










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versão impressa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.5 Madrid Mai. 2017
PICTURES IN DIGESTIVE PATHOLOGY
Esophageal perforation by a Sengstaken balloon
Perforación esofágica por balón de Sengstaken
Antonio José Fernández-López, María Encarnación Tamayo-Rodríguez, Francisco Miguel González-Valverde and Antonio Albarracín-Marín-Blázquez
Department of Surgery. Hospital General Reina Sofía. Murcia, Spain
Case report
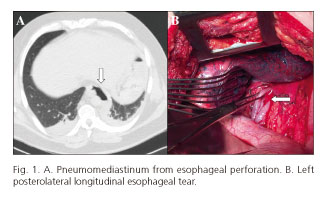
A 55-year-old patient presented with ethanolic cirrhosis (CHILD B9) and hemodynamic instability (heart rate: 112 bpm, blood pressure: 83/62) from massive upper gastrointestinal bleeding (UGIB). Upper gastrointestinal endoscopy (UGIE) revealed active bleeding from esophageal varices. As sclerotherapy and band ligation failed to provide hemostasis; the decision was made to use a Sengstaken balloon (SB). The balloon was insufflated with 300 ml for the gastric channel and 200 ml for the esophageal channel. X-rays after insufflation showed the gastric balloon at the distal esophagus. A repeat UGIE procedure showed a laceration at the lower third of the esophagus. A CT scan revealed pneumomediastinum (Fig. 1A). Given his clinical instability, the patient was operated on immediately, and an 8-cm longitudinal esophageal rupture was found in the lower third (Fig. 1B), which underwent primary suture repair. She died after five days from hepatorenal syndrome.
Discussion
UGIB from esophageal varices in the setting of portal hypertension is a high mortality situation. Treatment with vasoactive drugs and endoscopic ligation is effective in 76-96% of cases (1). SB is an effective salvage option when the above fails to temporarily control bleeding (effectiveness up to 90%) (2), but morbidity and mortality remain high. Major complications include: bronchoaspiration, rupture, and esophageal necrosis (2).
SB placement must be checked with auscultation to detect air insufflation within the gastric cavity, misplacement being the primary cause of esophageal rupture.
Surgery is the treatment of choice for esophageal rupture. Conservative endoscopic management with Ovesco clips and self-expandable stents has been described for smaller tears (< 10 mm) in the absence of sepsis (3).
References
1. Nielsen TS, Charles AV. Lethal esophageal rupture following treatment with Sengstaken-Blakemore tube in management of variceal bleeding: A 10-year autopsy study. Forensic Sci Int 2012;222:19-22. DOI: 10.1016/j.forsciint.2012.05.024. [ Links ]
2. Lin CT, Huang TW, Lee SC, et al. Sengstaken-Blakemore tube related esophageal rupture. Rev Esp Enferm Dig 2010;102(6):395-6. DOI: 10.4321/S1130-01082010000600014. [ Links ]
3. György L, Attila P, Eszter M. Role of endoscopic clipping in the treatment of oesophageal perforations. World J Gastrointest Endosc 2016;8(1):13-22. DOI: 10.4253/wjge.v8.i1.13. [ Links ]
