










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 n.5 Madrid May. 2017
PICTURES IN DIGESTIVE PATHOLOGY
Adrenal metastasis of hepatocellular carcinoma diagnosed by endoscopic ultrasound-guided fine-needle aspiration of the right adrenal gland
Katja Serra1, Roger Llatjos2, Isabel Català2 and Joan B. Gornals1
1Endoscopy Unit. Department of Digestive Diseases. Hospital Universitari de Bellvitge-IDIBELL. Barcelona, Spain.
2Department of Pathology. Hospital Universitari de Bellvitge-IDIBELL. Barcelona, Spain
Case report
A 79-year-old woman with a chronic hepatitis C virus infection and compensated cirrhosis was found to have two 3-cm liver masses and one 3-cm mass in the right adrenal gland on a multidetector computed tomography (MDCT) scan. By radiological criteria she was diagnosed to have bifocal hepatocellular carcinoma (HCC), but the MDCT scan could not characterize the adrenal mass. The HCC was successfully treated with chemo-embolization. To continue studying the adrenal gland, a magnetic resonance imaging was performed with no radiological criteria of adenoma, pheochromocytoma was ruled out with urine analysis and, finally, a positron emission tomography showed hyper-metabolism of the mass. Due to the suspicion of malignancy, EUS-guided fine needle aspiration (FNA) was performed.
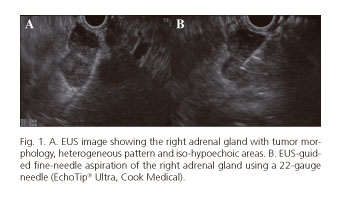
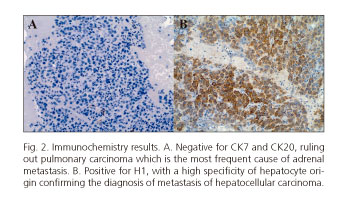
By using a linear echoendoscope the right adrenal gland was located in the side margin of the duodenal-pancreatic external frame, and showed a 3-cm tumor with a heterogeneous pattern (Fig. 1A). EUS-guided FNA was performed via trans-duodenal puncture using a 22-gauge needle. No immediate adverse events were related (Fig. 1B). Rapid on-site cytopathological evaluation and subsequent analysis of the sample confirmed the diagnosis of metastasis of HCC (Fig. 2A and B). Systemic chemotherapy with sorafenib was started with a good response.
Discussion
Recent studies have shown that the adrenal gland is the fourth most common site of HCC extrahepatic metastasis; despite this, the incidence of right adrenal metastasis of HCC is unclear (1).
EUS-guided FNA of the right adrenal gland is technically possible and safe, and should be considered in cases of right adrenal tumors with no diagnostic criteria by imaging tests (2,3).
References
1. Uchino K, Tateishi R, Shiina S, et al. Hepatocellular carcinoma with extrahepatic metastasis: Clinical features and prognostic factors. Cancer 2011;117:4475-83. DOI: 10.1002/cncr.25960. [ Links ]
2. Eloubeidi MA, Black KR, Tamhane A, et al. A large single-center experience of EUS-guided FNA of the left and right adrenal glands: Diagnostic utility and impact on patient management. Gastrointest Endosc 2010;71:745-53. DOI: 10.1016/j.gie.2009.10.022. [ Links ]
3. Eloubeidi MA, Morgan DE, Cerfolio RJ, et al. Transduodenal EUS-guided FNA of the right adrenal gland. Gastrointest Endosc 2008;67:522-7. DOI: 10.1016/j.gie.2007.10.031. [ Links ]
