










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.6 Madrid jun. 2017
PICTURES IN DIGESTIVE PATHOLOGY
A bronchobiliary fistula due to a giant hydatid cyst
Marcello Di Martino, Claudio Laganá, Jesús Delgado Valdueza and Elena Martín-Pérez
Hospital Universitario de La Princesa. Madrid, Spain
Case report
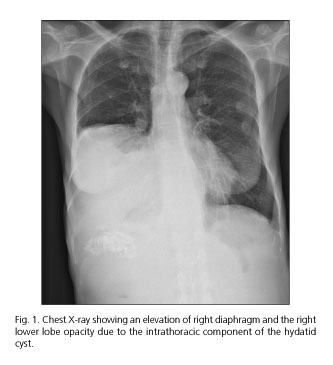
A 55-year-old female patient presented to the outpatient clinic due to chronic cough and biliptysia with hydatid debris expectoration during previous two months duration. Physical examination revealed a decrease in breath sounds in the right chest and palpable hepatomegaly. An indirect hemagglutination test was positive for anti-Echinococcus antibodies. A chest X-ray showed an elevation of the right diaphragm and right lower lobe opacity due to the intrathoracic component of the hydatid cyst (Fig. 1). An abdominal magnetic resonance imaging test showed a giant multiseptated hepatic cyst which was consistent with a hydatid cyst type CE 2 based on the World Health Organization (WHO) classification, which communicated with the biliary tree (Fig. 2) with massive extension to the right hemithorax (Fig. 3).


The patient was given 400 mg of albendazone every 12 hours and underwent abdominal surgery, which consisted of a pericystectomy of the giant hydatid cyst with evacuation of cyst debris from the bile duct, closure of hepatobronchial fistula, and repair of the diaphragm.
Discussion
Intrathoracic rupture of a hydatid cyst of the liver is a rare but severe complication of echinococcal disease with an incidence of around 1% and a mortality rate of approximately 10% (1). Early diagnosis and management of septic associated complications are essential (2). Surgery represents the definitive treatment with four main goals: treating the hydatid disease, assuring a free drainage of bile through the common bile duct, and closure of the hepatodiaphragmatic communication and of the tracheobronchial fistula (3). In cases of a simultaneous rupture of the cyst into the lung and the biliary tree, the evacuation of cyst debris from the bile duct takes priority over other surgical interventions.
References
1. Tierris EJ, Avgeropoulos K, Kourtis K, et al. Bronchobiliary fistula due to echinococcosis of the liver. World J Surg 1977;1(1):99-104. DOI: 10.1007/BF01654744. [ Links ]
2. Mihmanli M, Idiz UO, Kaya C, et al. Current status of diagnosis and treatment of hepatic echinococcosis. World J Hepatol 2016;8(28):1169-81. DOI: 10.4254/wjh.v8.i28.1169. [ Links ]
3. Tocchi A, Mazzoni G, Miccini M, et al. Treatment of hydatid bronchobiliary fistulas: 30 years of experience. Liver Int 2007;27(2):209-14. DOI: 10.1111/j.1478-3231.2007.01435.x. [ Links ]
