










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.10 Madrid oct. 2017
https://dx.doi.org/10.17235/reed.2017.5150/2017
CASE REPORT
Hepatocolic fistula managed with a novel Padlock® device for endoscopic closure
Fístula hepatocólica tratada con el nuevo dispositivo de cierre endoscópico Padlock®
Benito Velayos-Jiménez1, Lourdes del-Olmo-Martínez1, Carmen Alonso-Martín1, Javier Trueba-Arguiñarena2 and José Manuel González-Hernández1
Departments of 1Digestive Diseases and 2Radiology. Hospital Clínico de Valladolid. Valladolid, Spain
ABSTRACT
Recent advances in endoscopic therapeutics allow conditions such as fistulas of the digestive system to be treated endoscopically. These cases were recently managed with surgery. The Padlock® system includes a nitinol clip that was recently introduced for endoscopic therapy. There are few reports with regard to its use in the daily clinical practice. We report a case of a colonic fistula that was endoscopically managed with this novel over-the-scope nitinol clip system.
Key words: Therapeutic endoscopy. Over-the-scope clip. Fistula closure.
RESUMEN
El avance de la terapéutica endoscópica está permitiendo abordar patologías que hasta hace poco quedaban reservadas al tratamiento quirúrgico, como las fístulas digestivas.
El sistema Padlock® consiste en un clip de nitinol introducido recientemente para terapéutica endoscópica. Hasta el momento, son pocas las comunicaciones sobre su utilización en la práctica diaria. Presentamos un caso de fístula colónica tratada mediante este nuevo sistema de clip endoscópico de nitinol.
Palabras clave: Endoscopia terapéutica. Clip endoscópico. Cierre de fístula.
Case Report
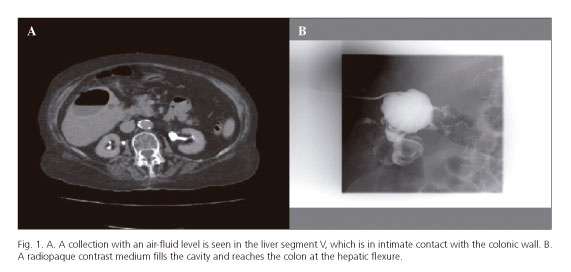
We report the case of a 92-year-old woman with a history of high blood pressure and temporal arteritis, under treatment with lisinopril and prednisone. The patient presented to the Emergency Room with fever and pain in the right upper quadrant of the abdomen of seven days duration. She had mild pain on deep palpation of the right hypochondrium. An abdominal CT scan was performed which revealed a calcified hydatid cyst and a 6 cm focal lesion with an air-fluid level consistent with a liver abscess in liver segment V. The latter lesion was in intimate contact with the hepatic angle of the colon (Fig. 1A). A percutaneous drain was placed by the Interventional Radiology Department, which allowed purulent material to be removed and contrast medium to be introduced into the cavity. No communication was found with the bile duct but the contrast reached the colon hepatic flexure (Fig. 1B). The initial clinical symptoms persisted after radiologic drainage, and cultures of the fluid collected from the lesion were positive for Eschericia coli and Streptococcus constellatus.
The fistulous tract observed by the radiographic study was confirmed by colonoscopy. The scan revealed a 7-8 mm fistulous orifice at the hepatic flexure which was 60 cm away from the anal margin with detritus discharge (Fig. 2A). The drain bag immediately filled with air upon air insufflation within the area. No diverticula were observed. Once specific consent was obtained, a Padlock Clip™ (Aponos Medical, Kingston, NH, United States) of the Pro-Select™ model (11 mm in diameter) was mounted on the tip of an Olympus GIF 1TQ160 video-gastroscope. Once the lesion was localized (Fig. 2B), the surrounding mucosa was aspirated into the plastic cap. The metallic endoclip was then released by gently pressing on the handle designed for this purpose. The metallic ring closed the colonic defect, leaving a mucosal pseudopolyp behind (Fig. 2C). Subsequently, the external drain was opened and air no longer passed into the bag attached to the radiologic drain. Complete closure of the fistulous tract was confirmed by a CT scan (Fig. 2D). The patient remained asymptomatic with no further drainage and was discharged from hospital after a seven day course of antibiotic therapy.

Discussion
The development of novel mechanical endoscopic closure systems allows for the management of some gastrointestinal fistula types in an effective, simple and safe manner (1). A new device was recently introduced with improved and appealing characteristics (2,3). Although similar in concept to the Ovesco® clip design, the setup is different, it does not involve the working channel and allows improved cleaning and aspiration. This system does not include forceps and suction is only used to introduce tissue into the cap before release (4). The new clip consists of an 11-mm hexagonal nitinol ring with six inner needles; the whole assembly lies within a plastic cap that is then fitted to the tip of the endoscope. Once the lesion is localized, the tissue in the target area is introduced into the cap by aspiration and the clip is then released by pressing a plastic push button (the Lock-it™ delivery system) at the end of a wire running externally along the shaft of the endoscope. Two cap models are available: a standard cap for endoscopes 9.5-11 mm in diameter and a Pro-Select™ cap for endoscopes 11.5-14 mm in diameter. Aspirated specimen depth may vary from 8 mm to 20 mm.
The high elasticity conferred by nitinol to the endoclip pushes the six inner prongs into the suctioned portion, thus closing the defects or bleeding points. On release, a pseudopolyp is formed above the clip. A high resistance to air pressure has been reported in porcine models, reaching up to 68 mmHg (5). The clip is radiopaque and its placement does not contraindicate subsequent MRI scans.
Reports on its use in daily practice are scarce and there are some heterogeneous series that have studied its location and applications (2,4,6,7). The system has been primarily used to control relapsed bleeding and for closing perforations or fistulae at various levels. To our knowledge, this is the first case to report the use of the system for the treatment of a fistula in the proximal colon.
Hepatocolic fistulas are uncommon and usually originate from collections communicating with the bile duct (8). They may also develop secondary to a pyogenic abscess (9). There is no well-defined protocol for clinical management, likely due to their unusual nature. Some authors recommend conservative measures with or without a radiographic procedure using drains. Other options should be considered for persistent clinical scenarios.
Each fistula or digestive wall defect must be approached on an individual basis according to clinical status and patient comorbidity. Etiology, characteristics and location should also be taken into account. The development of novel endoscopic closure mechanisms is changing the classic paradigm with regard to the need for surgery as a therapeutic option (10). Its main advantage is the ability to close the GI orifice using a minimally invasive approach with a lower morbidity. The procedure's simplicity is particularly valued by endoscopists, as with the Padlock® system used in this patient. Placement was straightforward using an endoscope, the hepatic flexure of the colon was reached, the view provided by the cap was adequate and the working channel was free to provide efficient washes and aspirations.
Although further endoscopies were not performed to check the status of the mucosa at the site of the pseudopolyp formed on fistula closure, the clip does not seem to induce ischemic problems. Further studies are needed to confirm the efficacy and safety of the novel Padlock® system for endoscopic closure. Easy over-the-scope assembly and release is a factor to be considered when using this device.
References
1. Takeshita N, Ho KY. Endoscopic closure for full-thickness gastrointestinal defects: Available applications and emerging innovations. Clin Endosc 2016;49(5):438-43. DOI: 10.5946/ce.2016.104. [ Links ]
2. Dinelli M, Omazzi B, Andreozzi P, et al. First clinical experiences with a novel endoscopic over-the-scope clip system. Endoscopy International Open 2017;05:E151-6. DOI: 10.1055/s-0043-101692. [ Links ]
3. Guarner-Argente C, Córdoba H, Martínez-Palli G, et al. Yes, we can: Reliable colonic closure with the Padlock-G clip in a survival porcine study. Gastrointest Endosc 2010;72:841-4. DOI: 10.1016/j.gie.2010.06.054. [ Links ]
4. Armellini E, Crino SF, Orsello M, et al. Novel endoscopic over-the scope clip system. World J Gastroenterol 2015;21:13587-92. DOI: 10.3748/wjg.v21.i48.13587. [ Links ]
5. Desilets DJ, Romanelli JR, Earle DB, et al. Gastrotomy closure with the lock-it system and the Padlock-G clip: A survival study in a porcine model. J Laparoendosc Adv Surg Tech Part A 2010;20:671-6. DOI: 10.1089/lap.2010.0076. [ Links ]
6. Schmidt A, Bauerfeind P, Gubler C, et al. Endoscopic full-thickness resection in the colorectum with a novel over-the scope devide: First experience. Endoscopy 2015;47:76-9. [ Links ]
7. Brindley JH, Yip B, Vlachou E, et al. Successful endoscopic closure of a gastrocutaneous fistula using a Padlock Clip. Endoscopy 2016;48:E115-6. DOI: 10.1055/s-0042-103422. [ Links ]
8. Velayos B, Prieto JM, Fernández L, et al. M. Fístula colecistocolónica diagnosticada por colonoscopia en una paciente asintomática. Med Clin 2013;140(9):432. DOI: 10.1016/j.medcli.2013.01.017. [ Links ]
9. Timbol AB, Mondragón KA, Banez VP. Hepatocolic fistula: A rare presentation of pyogenic liver abscess. BMJ Case Reports 2017. DOI: 10.1136/bcr-2016-219141. [ Links ]
10. Winder JS, Pauli EM. Comprehensive management of full-thickness luminal defects: The next frontier of gastrointestinal endoscopy. World J Gastrointest Endosc 2015;7(8):758-68. [ Links ]
![]() Correspondence:
Correspondence:
Benito Velayos-Jiménez.
Department of Digestive Diseases.
Hospital Clínico de Valladolid.
Av. Ramón y Cajal, 3.
47003 Valladolid, Spain
e-mail: benitovelayos@hotmail.com
Received: 03-07-2017
Accepted: 27-07-2017
