










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.11 Madrid nov. 2017
https://dx.doi.org/10.17235/reed.2017.4949/2017
The endoscopic ultrasound-assisted Rendez-Vous technique for treatment of recurrent pancreatitis due to pancreas divisum and ansa pancreatica
Tratamiento de pancreatitis recidivante por páncreas divisum y ansa pancreática mediante técnica de Rendez-Vous guiada por ecoendoscopia
Sergio López-Durán, Celia Zaera, Juan Ángel González-Martín, José Ramón Foruny, Agustín Albillos and Enrique Vázquez-Sequeiros
Endoscopy Unit. Gastroenterology Department. Hospital Universitario Ramón y Cajal, IRYCIS. Universidad de Alcalá. Alcalá de Henares, Madrid. Spain
ABSTRACT
Endoscopic treatment of pancreatic ductal malformations causing recurrent acute pancreatitis, such as pancreas divisum or ansa pancreatica, is mainly based on the sphincterotomy of the minor papilla. However, the technical complexity of conventional endoscopic retrograde cholangiopancreatography (ERCP) is increased in patients presenting anatomical variants like these and it may be unsuccessful. We report the case of a pancreas divisum combined with ansa pancreatica and describe the cannulation and sphincterotomy of the minor papilla using an ultrasound-assisted Rendez-Vous technique.
Key words: Pancreatitis. Rendez-Vous. Treatment. Endoscopic ultrasound.
RESUMEN
El tratamiento endoscópico de malformaciones ductales pancreáticas causantes de pancreatitis aguda de repetición, como el páncreas divisum o el ansa pancreática, se basa fundamentalmente en la esfinterotomía de la papila minor. En estos casos, no obstante, la complejidad técnica de la colangiopancreatografía endoscópica retrógrada (CPRE) convencional es mayor, pudiendo resultar fallida. Presentamos el caso de un páncreas divisum completo combinado con ansa pancreática, sintomático, en el que, tras fracasar el acceso endoscópico convencional a la papila minor, se logra la canulación y esfinterotomía de esta mediante técnica de Rendez-Vous guiada ecoendoscópicamente.
Palabras clave: Pancreatitis. Rendez-Vous. Tratamiento. Ecoendoscopia.
Introduction
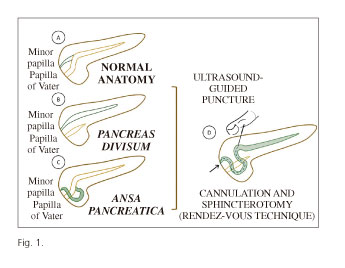
The cornerstone for treatment of symptomatic pancreas divisum is the decompression of minor duodenal papilla by sphincterotomy (1), which has also served for the treatment of other less frequent ductal malformations of the pancreas such as ansa pancreatica (2). The latter consists of an additional arcuate branch that connects the dorsal and ventral ducts that is associated with a proximal obstruction of the accessory pancreatic duct (Fig. 1). Endoscopic access to minor papilla in patients presenting anatomical variants such as these increases the technical difficulty and probability of failure, even more so if combined. As conventional endoscopic treatment by endoscopic retrograde cholangiopancreatography (ERCP) may be unsuccessful in these and other situations of a similar nature, an endoscopic ultrasonography-guided access could be attempted in order to achieve the cannulation and sphincterotomy of the minor papilla by the Rendez-Vous technique (3).
Case Report
We report the case of a 72-year-old man with a well-documented history of recurrent acute pancreatitis due to a pancreas divisum combined with ansa pancreatica (Fig. 1D). This anatomical abnormality was diagnosed by abdominal magnetic resonance imaging (MRI) and confirmed by endoscopic ultrasonography (EUS). The patient was referred to our center for endoscopic treatment (minor papilla sphincterotomy) after two failed attempts using conventional ERCP.
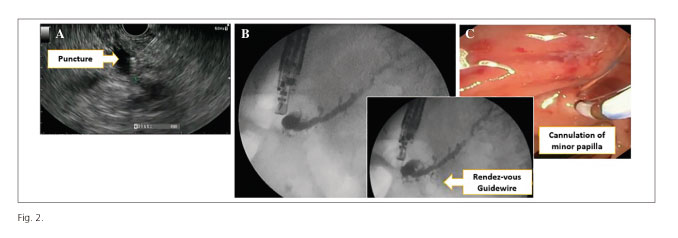
The pancreatic gland was initially examined using an echoendoscope. The accessory duct ran in a curved manner (ansa) from the minor papilla to the main pancreatic duct, which in turn had a retrograde dilation of 5 mm. As the initial cannulation attempt of the papilla minor was unsuccessful, insertion using a Rendez-Vous technique was attempted. The procedure began with a transgastric ultrasound-assisted puncture into the ansa with a 19G needle (Figs. 1D and 2A) and the known anomaly was confirmed by a pancreatogram (Fig. 2B). Subsequently, a 0.021 inch guidewire was introduced and advanced toward the minor papilla through the ansa. When the duodenal lumen was reached, the echoendoscope was removed and a duodenoscope inserted parallel to the guidewire. Biopsy forceps were introduced using a Rendez-Vous technique through the instrumental channel of the duodoscope in order to pull the widewire out from the duodenum and finally achieve a guidewire-assisted cannulation of the minor papilla (Fig. 2C). The guidewire was then removed until it reached the tip of the sphincterotome DASH-21-480 (Cook®) and moved again toward the pancreas tail (Figs. 3 A and B). At this point, a sphincterotomy of the minor papilla was performed and a pancreatic stent (a 5 Fr, 5 cm straight plastic stent with side flaps) was inserted endoscopically in order to ensure pancreatic drainage and prevent acute pancreatitis.

Discussion
Pancreas divisum is the most common congenital variant of the pancreatic duct system and is present in up to 10% of the population according to some studies (4). Nevertheless, it is mostly asymptomatic. This entity occurs due to the lack of fusion of the ventral and dorsal pancreatic ducts during embryological development. Therefore, the dorsal duct must drain the majority of the pancreas into the minor papilla (5).
Ansa pancreatica malformation is considered as another congenital variant in the anatomy of the pancreatic duct system. It is called ansa (in Latin this means "handle") because of its curved morphology. It consists of an aberrant branch that arises from the main pancreatic duct and disembogues into the minor papilla, forming a loop with caudal convexity. (6) (Fig. 1C).
The duct of Santorini (accessory pancreatic duct) produces a decompressive effect on the duct of Wirsung (main pancreatic duct) in a normal pancreatic duct system. However, patients with pancreas divisum and/or ansa pancreatica would hypothetically have an inadequate drainage of the pancreatic duct system and consequently have a relative increase of intraductal pressure into the main pancreatic duct. This has been suggested as a causative factor of pancreatitis (6,7).
Due to the aforementioned, endoscopic treatment of pancreas divisum (or more rarely treatment of ansa pancreatica [2]) is based on minor papilla decompression, mainly by sphincterotomy. This therapeutic option has been shown to be more effective in patients with acute recurrent pancreatitis than in other clinical settings (9,10).
Isolated endoscopic cannulation of the minor papilla may be technically challenging. As presented above, any combination of different types of ductal abnormalities further increases this complexity. Therefore, the introduction and movement of the guidewires into the duct system may become a great challenge (Fig. 1D). In this report, we describe for the first time an endoscopic approach for the cannulation of the minor papilla via the ansa, using an ultrasound-assisted Rendez-Vous technique. However, this is actually considered as a "typical" indication for this kind of procedure, specifically, pancreatic drainage abnormalities with clinical impact and previous failed ERCP attempts (3,10). Even though this is not the most common indication in clinical practice, it is important to keep it in mind as a therapeutic option in complicated cases.
In conclusion, when performed by expert endoscopists, therapeutic endoscopic ultrasonography is an effective and safe pancreatic drainage option in complex cases where conventional endoscopic procedures have failed.
References
1. Riff PB, Chandrasekhara V. The Role of Endoscopic Retrograde Cholangiopancreatography in Management of Pancreatic Diseases. Gastroenterol Clin North Am 2016;45:45-65. DOI: 10.1016/j.gtc.2015.10.009. [ Links ]
2. Bhasin DK, Rana SS, Nanda M, et al. Ansa Pancreatica Type of Ductal Anatomy in a Patient with Idiopathic Acute Pancreatitis. J Pancreas 2006;7:315-20. [ Links ]
3. Prachayakul V, Aswakul P. Endoscopic ultrasound-guided interventions in special situations. World J Gastrointest Endosc 2016;8:104-12. DOI: 10.4253/wjge.v8.i2.104. [ Links ]
4. Lehman GA, Sherman S. Diagnosis and therapy of pancreas divisum. Gastrointest Endosc Clin N Am 1998;8:55-77. [ Links ]
5. Saltzman JR. Endoscopic treatment of pancreas divisum: why, when and how? Gastrointest Endosc 2006;64:712-5. [ Links ]
6. Kamisawa T, Takuma K, Tabata T, et al. Clinical implications of accessory pancreatic duct. World J Gastroenterol 2010;16:4499-503. DOI: 10.3748/wjg.v16.i36.4499. [ Links ]
7. Jarrar MS, Khenissi A, Ghrissi R, et al. Ansa Pancreatica: an anatomic variation and a rare cause of acute pancreatitis. Surg Radiol Anat 2013;35:745-8. DOI: 10.1007/s00276-013-1103-7. [ Links ]
8. Lans J, Geenen J, Johanson J, et al. Endoscopic therapy in patients with pancreas divisum and acute pancreatitis: a prospective, randomized, controlled clinical trial. Gastrointest Endosc 1992;38:430-4. DOI: 10.1016/S0016-5107(92)70471-4. [ Links ]
9. Heyries L, Barthet M, Delvasto C, et al. Long-term results of endoscopic management of pancreas divisum with recurrent acute pancreatitis. Gastrointest Endosc 2002;55:376-81. DOI: 10.1067/mge.2002.121602. [ Links ]
10. Rana SS, Gonen C, Vilmann P. Endoscopic ultrasound and páncreas divisum. J Pancreas 2012;13:252-7. [ Links ]
![]() Correspondence:
Correspondence:
Enrique Vazquez-Sequeiros.
Endoscopy Unit.
Gastroenterology Department.
Hospital Universitario Ramón y Cajal, IRYCIS.
Ctra. Colmenar Viejo, km. 9,100,
28034 Madrid, Spain
e-mail: evazquezse@gmail.com
Received: 14-03-2017
Accepted: 14-07-2017
