










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Cirugía Oral y Maxilofacial
On-line version ISSN 2173-9161Print version ISSN 1130-0558
Rev Esp Cirug Oral y Maxilofac vol.29 n.4 Madrid Jul./Aug. 2007
ARTÍCULO CLÍNICO
A new indication for Zygomatic implants for the fixed rehabilitation of the partially edentulous patient: Case report
Nueva indicación de implantes cigomáticos para la rehabilitación fija de desdentados parciales: reporte de un caso
M.F. Pintor Willcock1, O. Campos Salvaterra2
1 Cirujano-Dentista. Becado en formación académica
Clínica Alemana de Santiago. Cátedra de Cirugía Oral. Facultad de
Oodntología.
Universidad Mayor, Chile.
2. Cirujano-Dentista. Cirujano Máxilo-facial
Servicio de Cirugía Máxilo-facial Clínica Alemana de Santiago. Servicio de
Cirugía Máxilo-facial Hospital José Joaquin Aguirre. Postgrado de
Implantología.
Facultad de Odontología. Universidad de Chile. Chile.
ABSTRACT
Zygomatic Implants are used in the rehabilitation of severely resorbed maxillas. This eliminates the necessity of bone grafting or sinus augmentation to restore the osseous volume necessary for conventional implant rehabilitation. This also minimizes morbidity and treatment times. We present the case of a patient with a partially edentulous upper ridge, Kennedy class I, in whom two zygomatic implants were placed in each side, that emerged over the alveolar ridge crest as a result of a technique modification.
Key words: Zygomatic Implants; Dental Implants; Maxilla; Zygoma; Oral Rehabilitation.
RESUMEN
Los implantes cigomáticos están indicados en casos de reabsorciones maxilares severas. Esto permitiría eliminar la necesidad de injertos óseos o levantamientos de seno de manera de recuperar el volumen óseo necesario para rehabilitar en base a implantes convencionales, disminuyendo así la morbilidad y el tiempo de tratamiento. A continuación presentamos caso de paciente desdentado parcial superior, clase I de Kennedy, en el cual se utilizaron dos implantes cigomáticos a cada lado, emergiendo sobre el reborde, a través de una modificación de la técnica.
Palabras clave: Implantes cigomáticos; Implantes dentales; Maxilar; Cigoma; Rehabilitación oral.
Introduction
The zygomatic implants created and developed by Dr. Branemark have been used as posterior anchors for implantsupported prostheses in patients with severe resorbed maxillae, since 1990.1-3 The original concept established the placement of a single implant in the zygoma, bilaterally, combined with at least two conventional implants in the anterior sector of the maxilla. 3,4 Historically, a series of procedures have been described for treating the atrophic maxilla, such as sinus elevation, onlay bone grafts, bone grafts combined with Lefort I osteotomies; which have provided adequate bone volume for the installation of implants.1,2,5,6 These treatment options include a series of procedures and the need for hospitalization and obtaining bone for distant sites, such as iliac crest of calvarial bone.2,5 These additional procedures have led to their rejection by many patients because of the high morbidity this entailed.5 A treatment alternative for this group of patients are zygomatic implants, which are titanium endosseous implants, between 30 and 52.5 mm in length. The implant is introduced in the area of the second premolar, it crosses the maxillary sinus and is fixed to the body of the malar. By fixing a minimum of two premaxillary implants in the area of the canines, or 4 in the central incisor area, hybrid prostheses can be made.3-5
Clinical case
Edentulous female patient, 55 years old, with a partial upper class I Kennedy with the remains of teeth 6 to 12 in her mouth. She requested at her consultation the rehabilitation of the posterior region. In accordance with the radiographic study, she had considerable bilateral resorption because of pneumatization of the maxillary sinus. As a result of this, reconstruction with a calvarial graft and implants in a second surgical stage was planned. This treatment was rejected because of high morbidity. For this reason, rehabilitation was planned based on zygomatic implants, to replace the area up to the first molar. For this, two zygomatic implants were placed at each side, three that measured 45 mm and one of 40 mm.
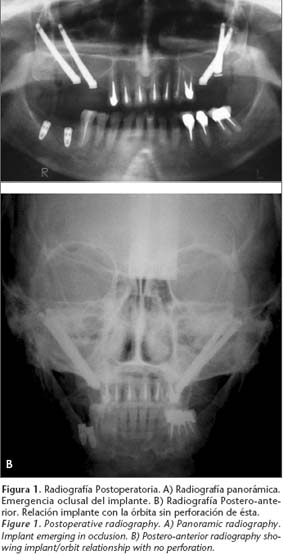
For a fixed prosthesis type rehabilitation the implants needed to emerge from the alveolar crest, and because of this the original technique was modified. The implants on the right side were placed by teeth 3 and 4. The posterior implant was situated outside the maxillary sinus and the anterior implant on the inside, but at a greater angle with regard to the occlusal plane. On the left side, by teeth 13 and 14, the anterior implant was positioned outside the maxillary sinus and the posterior implant on the inside at a greater angle (Figs. 1 and 2). With this the four implants were able the emerge from the alveolar ridge (Fig. 3) at an angle that was within acceptable limits (Fig. 4).



Discussion
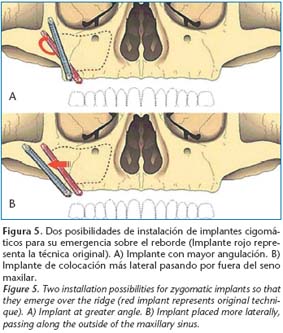
The use of zygomatic implants avoids the need for using bone grafts and treatment times are shorterned.2 The original protocol describes placing a zygomatic implant on each side, always within a rehabilitation plan for totally edentulous patients, principally due to the disadvantage that according to the original technique, of situating the implant platform in the palate.1,4,7 This generates biomechanical problems that permit rehabilitation based only on hybrid fixed prostheses, leading to hygiene problems and in some cases articulation problems. Many modifications of this technique have been described.3,6,7 In this case we present two possibilities that permit placing the zygomatic implant in a position where it emerges from the alveolar ridge. This permits rehabilitation based on conventional fixed prostheses in partially edentulous patients, as in this case of ours. The first option consists in introducing the implant outside the maxillary sinus and another option would be to introduce it at a greater angle, placing it in a more vertical position, in such a way that it emerges through the ridge (Fig. 5), always taking into account the relationship between the end of the implant and the orbit.
While the instruments necessary for placing
zygomatic implants are designed for totally edentulous patients, with a greater
installation space and at a particular angle, developing the technique in
partially edentulous patients with the remains of anterior dental groups, is
made more difficult. This is mainly to do with the length of the drills.
However, we believe that this technique modification can be developed without
any major complications, thus widening the spectrum for the indications of
Zygomatic Implants, with very good results.
![]() Correspondence:
Correspondence:
María Fernanda Pintor Willcock
Charles Hamilton 10038, Santiago, Chile
Email: fernandapintor@gmail.com
Recibido: 12.09.06
Aceptado: 01.06.07
References
1. Nakai H, Okazaki Y, Ueda M. Clinical application of zygomatic implants for rehabilitation of the severely resorbed maxilla: A Clinical Report. Int J Oral Maxillofac Implants 2003;18: 566-70. [ Links ]
2. Nkenke E, Hahn M, Lell M, y cols. Anatomic site evaluation of the zygomatic bone for dental implant placement. Clin Oral Impl Res 2003; 14:72-9. [ Links ]
3. Bothur S, Jonsson G, Sandahl L. Modified technique using multiple zygomatic implants in reconstruction of the atrophic maxilla: A Technical Note. Int J Oral Maxillofac Implants 2003;18:902-4. [ Links ]
4. Uchida Y, Goto M, Katsuki T, Akiyoshi T. Measurement of the maxilla and zygoma as an aid in installing zygomatic implants. J Oral Maxillofac Surg 2001;59:1193-8. [ Links ]
5. Bedrossian E, Stumpel L, Beckely M, Indersano T. The zygomatic implant: preliminary data ontreatment of severely resorbed maxillae. A clinical report. Int J Oral Maxillofac Implants 2002;17:861-5. [ Links ]
6. Boyes-Varley JG, Howes DG, Lownie JF, Blackbeard GA. Surgical Modifications to the Brånemark Zygomaticus Protocol in the Treatment of the Severely Resorbed Maxilla: A Clinical Report. Int J Oral Maxillofac Implants 2003;18:232-7. [ Links ]
7. Stella JP, Warner MR. Sinus slot technique for simplification and improved orientation of zygomaticus dental implants: a technical note. Int J Oral Maxillofac Implants 2000;15:889-93. [ Links ]

