










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Cirugía Oral y Maxilofacial
versión On-line ISSN 2173-9161versión impresa ISSN 1130-0558
Rev Esp Cirug Oral y Maxilofac vol.31 no.6 Madrid nov./dic. 2009
Surgical Treatment for Masseteric Hypertrophy: Case Report with Six-year Follow-up
Tratamiento quirúrgico de hipertrofia maseterina: Reporte de un caso con seguimiento de seis años
N. Yanine1, I. Araya1, M. Cornejo2,3, J. Villanueva1,2
1 Departamento de Cirugía y Traumatología Máxilo Facial. Facultad de Odontología. Universidad de Chile. Santiago, Chile.
2 Servicio de Cirugía Máxilo Facial. Hospital Clínico San Borja Arriarán. Chile.
3 Departamento de Radiología. Facultad de Odontología. Universidad de Chile. Chile.
ABSTRACT
Masseteric hypertrophy is a benign condition that can be appear in an asymmetric or symmetric form. Aesthetics is the main problem. Many treatments have been proposed, the surgical alternative is the most predictable and radical. We present the case of a 15 year-old girl with asymmetric masseteric hypertrophy who is surgically treated and then monitored for 6 years without recurrences.
Key words: Masseteric hypertrophy; Asymmetric face; Masseter.
RESUMEN
La hipertrofia maseterina es una condición benigna que puede manifestarse en forma bilateral o unilateral. Presenta como principal problema el componente estético. Se han planteado diversos tratamientos, siendo la alternativa quirúrgica la más radical y predecible. Se presenta el caso de una adolescente de 15 años que presentó hipertrofia maseterina unilateral, la cual fue tratada en forma quirúrgica y fue controlada durante 6 años sin recidivas.
Palabras clave: Hipertofia maseterina; Asimetría facial; Masetero.
Introduction
Masseteric hypertrophy is a benign condition that can be asymptomatically appear in an asymmetric or symmetric form. This condition has an unclear etiology and comes from functional conditions of the individual. In most cases, the consult is because aesthetic reasons, due to the increased volume of the involved region that can also be accompanied by a mandible angle exostosis. This condition is generally found in young patients who use a night guard or chewing gum and are under stress which can cause masseteric hyperactivity. It has also been related with the use of anabolic substances.1
Its diagnosis can be confused with other pathologies such as: parotiditis, benign muscle tumor or vascular lesions causing a volume increase of this region, so a comprehensive clinical examination is needed.2 Many treatments have been proposed from less invasive measures like muscle relaxers, mouth guards and botulinic toxins to more drastic measures like surgery. The proposed treatment has suggested low invasive measures such as muscle relaxants, mouth guards, botulinic toxin and surgery.2
The case of a patient with asymmetric masseteric hypertrophy surgically treated by extra oral resection of mandible angle is presented.
Clinical case
At the Unit of Maxillofacial Surgery at San Borja Arriarán Hospital, a 15 year old female patient went to the doctor because of a painless right facial asymmetry progressively appearing without other symptoms.
During the consultation, the patient does not report a morbid or surgical background, use of pharmaceuticals, allergies or other type of malfunctioning.
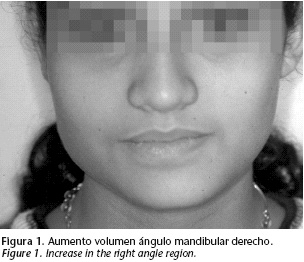
During the extra oral examination, an increase in the right angle region is observed, with unclear limits, hard and painless at palpation (Fig. 1). During palpation we could not observe inflammatory signs, or compromise of the sub mandible or cervical gland. The TMJ (Temporomandibular Joint) exam did not show pathological signs or symptoms.
The intra oral examination does not show any significant signs regarding soft tissues, denture or occlusion. Salivary secretion is normal, particularly in terms of the Stemson's ducts.
The panoramic x-ray showed a more marked right mandible angle (Fig. 2). The skull lateral x-ray showed a double mandible boundary and the frontal tele-x-ray showed that the mandible right area had a greater development without affecting the occlusal plane. An osseous scintigraphy and an electromyography were performed in order to eliminate the possibility of condyle hyperplasia. The diagnosis was a right asymmetric masseteric hypertrophy, which led to an extra oral resection of the right mandible angle.

Under general anesthesia, a mandible sub angle access is made to expose the ipsilateral angle. This angle and part of the masseteric muscle are resectioned. Biopsy of the resectioned muscle did not show any pathological condition of tissues.
The patient was immediately monitored after the surgery without complications. The patient was examined 6 years later and was in good condition without recurrences (Fig. 3).

Discussion
The masseteric hypertrophy has been described as a benign condition that can be presented in an asymmetric or symmetric form. Its etiology has not been well defined. Several acquired conditions have been proposed as the cause of appearance. The muscle volume increase can appear together with an exosthosis in the mandible angle region. Our patient had this condition which can be explained as the soft tissues' response to this high caliber muscle. This condition does not mean an increase in the muscle electromyographic activity. Roncevic3 has demonstrated that in asymmetry cases the electromyographic activity is equal in both muscles. This condition is not an increase in the electromyographic activity of muscle but the force of such muscle is greater. Results were similar to those found in our electromyography.
Diagnosis can be confused with other pathologies,2 so a good interview and a clinical examination are crucial. The CAT (Computed Axial Tomography) and the nuclear magnetic resonance4 are very useful.
Regarding treatment, there are several documents that suggest the angle exosthosis resection (when it is appears) with partial masseter myotomy without considering the chosen access.5-10 Results are satisfactory and without recurrences, as showed in our case six years after surgery.
The partial excision of the masseter muscle resulted in a loss of muscle mass and part of the fibers surrounding this portion suffered atrophy causing the expected result.6-8 Recurrences can be expected if the etiological cause is not eliminated, but it will not happen because of atrophy. Lo, Mardini and Chen,11 after a 4 and a half year follow-up, measured the volume loss of masticatory muscles (internal, external pterygoid nerves and masseter) at the resection of mandible angles. They observed that volume changes were not significant but they were enough to determine an aesthetic improvement. They also found that the external pteryoid never had a volume increase because of a compensatory mechanism.
Muscle biopsy of the removed section showed completely normal muscle fibers, without hypertrophy or anomalies. This leads us to question if it is caused by hypertrophic tissues or by a muscle increase caused other factors. It's possible that in some cases the functional stimuli cause the volume increase (muscle fiber recruitment) and in other cases it is caused by genetic anomalies. This patient did not have any background involving a predisposition to develop a masseteric hypertrophy. Addante8 suggests that the masseteric hypertrophy constitute only a genetic condition since he found normal fibers in biopsies and suggests the "masseteric hyperplasia" as the more appropriate definition.
It is important to consider complications when carrying out the angular resection for example lower dentary nerve damage12 or masseteric artery hemorrhage.13 In this case, these complications were not and issue because of the access and cephalometries chosen to determine the quantity of angle to be extirpated.
At present, botulinic toxin is a new alternative that prevents the action of cholinergic terminals blocking the neuromuscular presynaptic impulses. Then new innervations are generated recovering the presynaptic activity. The habit that caused the hypertrophy is stopped because the muscle could not be activated during a period, thus maintaining the initial result.14
In our opinion, literature regarding the etiology on this pathology is unclear. Although the prognostic is good and surgical treatment results are steady in time, more studies are required for a deeper understanding of its nature.
![]() Correspondence:
Correspondence:
Dr. Nicolás Yanine Montaner
Departamento de Cirugía y Traumatología Máxilofacial
Facultad de Odontología, Universidad de Chile.
Olivos 973, Independencia, Santiago, Chile.
E-mail: nyanine@gmail.com
Recibido: 24.09.2008
Aceptado 25.08.2009
References
1. Skoura C, Mourouzis C, Saranteas T, Chatzigianni E, Tesseromatis C. Masseteric hypertrophy associated with administration of anabolic steroids and unilateral mastication: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;92:515-8. [ Links ]
2. Mandel L., Surattanont F. Bilateral parotid swelling: a review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;93:221-37. [ Links ]
3. Roncevic R. Masseter muscle hyperthrophy. Aethiology and therapy. J Maxillofac Surg 1986;14:344-8. [ Links ]
4. Seltzer S, Wang A. Modern imaging of the masseter muscle: normal anatomy and pathosis on CT and MRI. Oral Surg Oral Med Oral Pathol 1987;63:622-9. [ Links ]
5. Nishida M.,Iizuka T. Intraoral removal of the enlarged mandibular angle associated with masseteric hyperthrophy. J Oral Maxillofac Surg 1995;53:1476-9. [ Links ]
6. Wood G. Masseteric hyperthrophy and surgical correction. Br Dent J 1982;152:416-7. [ Links ]
7. Chee LF, Fei YJ. Surgical correction of masseter muscle hyperthrophy by an intraoral approach. J Oral Maxillofac Surg 1989;47:883-5. [ Links ]
8. Addante R. Masseter muscle hyperthrophy: report of case and literature review. J Oral Maxillofac Surg 1994;52:1199-2. [ Links ]
9. Yooho L, Jun Ho K. Mandibular contouring: a surgical technique for the asymmetrical lower face. Plast Recons Surg 1999;104:1165-1. [ Links ]
10. Deguchi M, Iio Y, Kobayashi K, Shirakabe T. Angle-splitting ostectomy for reducing the width of the lower face. Plast Recons Surg 1997;99:1831-9. [ Links ]
11. Lo L, Mardini S, Chen Y. Volumetric change of the muscles of mastication following resection of mandibular angles. A long term follow up. Ann Plast Surg 2005;54:615-1. [ Links ]
12. Lo LJ, Wong FW, Chen YR. The position of the inferior alveolar nerve at the mandibular angle: an anatomic consideration for aesthetic mandibular angle reduction. Ann Plast Surg 2004;53:50-5. [ Links ]
13. Hwang K, Kim Y, Chung I, Lee S. Deep middle masseteric artery attributed to hemorrhage in resection of masseter muscle and mandibular angle. J Craniofac Surg 2001;12:381-5. [ Links ]
14. Mandel L, Tharakan M. Treatment of unilateral masseteric hyperthrophy with botulinum toxin: a case report. J Oral Maxillofac Surg 1999;57:1017-9. [ Links ]

