










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIdiopathic toe-walkers (ITWs) are children with a usual tiptoe gait (Fox, Deakin, Pettigrew, & Paton, 2006), but they are capable of heel-striking when they are asked to or when their attention is drawn to it, with an absence of gastrosoleus retraction (Brunt et al., 2004; Stricker, 2006; Westberry, Davids, Davis, & de Morais, 2008). Idiopathic tip-toe gait is considered as an exclusion diagnosis in children older than 3 years (Engelbert, Gorter, Uiterwaal, van de Putte, & Helders, 2011; Williams, Tinley, Curtin, Wakefield, & Nielsen, 2013; Williams, Tinley, & Rawicki, 2014), once principal orthopedic and neurological conditions are discarded (Fox et al., 2006; Stricker, 2006). However, some authors have speculated that idiopathic tiptoe gait is a motor expression of a minimal cerebral dysfunction, as this kind of gait has been related to difficulties in psychomotricity, learning, behavior, speech, language, and sensory integration (Fox et al., 2006; Shulman, Sala, Chu, McCaul, & Sandler, 1997; Stricker, 2006; Williams, Tinley, Curtin, Wakefield et al., 2013; Williams et al., 2014). So, developmental evaluation is strongly recommended in ITW and a specific treatment could be implemented if necessary (Williams et al., 2014).
As biomechanical aspects, toghether with a progressive secondary triceps surae retraction in older children (Engelbert et al., 2011; Shulman et al., 1997; Williams, Tinley, Curtin, & Nielsen, 2013), compensations for long term tiptoe gait include valgus rearfoot, external tibial torsion, and an abducted gait pattern (McMulkin, Baird, Caskey, & Ferguson, 2006). For this reason, orthopedic evaluation is highly recommended (Williams, Tinley, Curtin, & Nielsen, 2013) and therapeutical approaches are focused on these alterations once stablished (van Kuijk, Kosters, Vugts, & Geurts, 2014). Some authors have studied kinetic and kinematic idiopatic toe-walking (ITW) gait characteristics to quantify them and Alvarez, Vera, Beauchamp, Ward, & Black (2007) have designed a specifical classification for ITW. They classified ITW in three progressive severity types by the presence of a first ankle rocker, an early third ankle rocker, and a predominant first ankle flexor moment. This classification has showed its usefulness to select the best treatment option and evaluate its effectiveness (Engström et al., 2010), but it has not been related with orthopedic or developmental ITW characteristics.
A dynamic pedobarographic analysis has been suggested for children gait evaluation because of its sensitivity to detect light changes (Alvarez, Vera, Chhina, & Black, 2008; Bertsch, Unger, Winkelmann, & Rosenbaum, 2004; Bosch, Gerss, & Rosenbaum, 2010; Hallemans, De Clercq, Van Dongen, & Aerts, 2006), but there is a lack of studies about ITW. It could be a valid instrument to reveal differential patterns of plantar pressure distribution in ITW, to indicate a therapeutical option (Bosch et al., 2010; Eiff, Steiner, & Zegar, 2006; Hallemans et al., 2006).
The aim of this work is to develop a dynamic pedobarographic classification in ITW, linking these models with orthopedic and developmental characteristics, to propose a specific therapeutical approach depending on them.
Method
One hundred and fifty-one children (3-6 years old) were recruited for this prospective research via specific advertising. Two experienced physiotherapists conducted a developmental, orthopedic, and dynamic pedobadographic analysis. The inclusion criteria of ITW were being currently toe-walkers and starting since gait began (Engström & Tedroff, 2012; Williams, Tinley, Curtin, & Nielsen, 2013; Williams, Tinley, Curtin, Wakefield et al., 2013). The exclusion criteria for ITW and control type (CG) included trauma disorders, neurological or developmental ones, unilaterally tiptoe gait, and previous treatment for tiptoe gait. According to these criteria, 96 children (56 ITWs and 40 in the CG) were selected out of those who fulfilled the inclusion criteria and whose parents had signed the informed consent. Excluded children were mostly affected by flatfeet, in-toeing gait, neurodevelopmental disorders, and inability to complete valuation. This observational study was previously approved by the Clinical Investigation Ethics Committee of the Faculty.
Dynamic Pedobarographic Analysis
Children's age, sex, height, and weight were firstly collected. Pedobarographic gait analysis was performed using Footscan USB Gait Clinical System® (2 m x 0.4 m x 0.02 m, 16,384 sensors, 500 Hz, and 3 sensors per cm2), embedded in a 9-meter walkway. Children were asked to walk onto the gait track at a comfortable speed and looking at the front, after they had been freely barefoot walking for a minute. At least 10 whole fingerprints of both feet were recorded and their average was considered for the analysis. The variables analyzed were calculated directly by the system by means of the automatic division in foot zones (Alvarez et al., 2008; Bertsch et al., 2004; Bosch et al., 2010; Crenna, Fedrizzi, Andreucci, Frigo, & Bono, 2005; Hallemans et al., 2006; Liu, Thometz, Tassone, Barker, & Lyon, 2004). The variables studied were peak pressure, percentage of impulse, total foot impulse, percentage of contact time, and step duration.
Low Extremity Orthopedic Assessment
Physical evaluation included the measure of the popliteal angle, the passive ankle dorsiflexion, both with extended and flexed knee, the relaxed calcaneal stance position, and the pronation angle. Angular measurements were obtained using a handheld goniometer, with modalities which have demonstrated to range from moderate to high reliability (Evans, Cooper, Scharfbillig, Scutter, & Williams, 2003; Van Gheluwe, Kirby, Roosen, & Phillips, 2002).
Developmental Evaluation
Developmental evaluation was performed by the Cuestionario de Madurez Neuropsicológica Infantil [Child's Neuropsychological Development Questionnaire] (CUMANIN), a very complete test validated in Spain that evaluates all aspects of children development and enables us to compare them with reference values for the chronological age (Portellano, Mateos, Martínez-Arias, Tapia, & Granados, 2000). Global and specific scales results can be expressed as farthings with respect to the reference population and all of them have been considered for this study, and also the global indicator known as Development Quotient. CUMANIN has been described as an useful tool for developmental evaluation of different Spanish children samples, both with and without disorders (Portellano, 2004; Portellano et al., 2000).
ITW Types Configuration
ITWs were classified through an analysis of their initial foot contact and the step development during dynamic pedobarographic analysis by means of the initial contact time for each foot zone (Figure 1). Type 1 (n = 23) included children who showed a clear inicial hindfoot strike progressively followed by midfoot and forefoot in a roller from heel to toes. Type 2 (n = 27) demonstrated an initial contact with the hindfoot together with other foot zones in a flatfoot contact, or a variable initial contact by the alternation of heel strike with the flatfoot contact. Type 3 (n = 6) included children who demonstrated an initial forefoot contact followed by a retrograde hindfoot contact.

Results
ITWs and CG showed similar anthropometric characteristics: age (CG = 56.55 ± 14.23 months; ITWs = 54.70 ± 12.17 months; p > .05), weight (CG = 18.56 ± 3.32 kg; ITWs = 19.56 ± 3.49 kg; p > .05) height (CG = 1.07 ± 0.09 m; ITW = 1.09 ± 0.08 m; p > .05) and body mass index (CG = 15.94 ± 1.25; ITWs = 16.46 ± 1.9; p > .05).
Significant differences were not found in demographic and anthropometric characteristics between ITW types except for weight (p = .03). Type 3 ITWs were the older children (58.17 ± 20.72 months); they were the heaviest (22.88 ± 3.36 kg) and the tallest (1.15 ± 0.1 m) with significant differences with CG (p = .022 and p = .023, respectively). The pedobarographic analysis is not biased by these results, as body mass did not significantly influence plantar pressure data in children in this age range (Phethean & Nester, 2012).
The right extremity was considered for the study, as the absence of significant differences between both feet has been demonstrated by another dynamic pedobarographic analysis in similar samples (Alvarez et al., 2008; Bosch et al., 2010; Phethean & Nester, 2012). Dynamic pedobarographic analysis demonstrated many significant differences between ITW types and with respect to the CG, to configurate three different ITW models of step development (Figure 1).
Peak pressure analysis demostrated significant differences between the three ITW types in the peak pressure exerted by the first metatarsal (p = .000) and the medial and lateral hindfoot zones (p = .013 and p = .01, respectively). Type 3 ITWs demonstrated a higher peak pressure exerted by the first metatarsal and lowest with the hindfoot, whereas Type 1 showed more similar values to CG in all zones except for the hallux and the midfoot (p < .05). In Type 2 the midfoot and the hindfoot exerted lower peak pressures than the CG and also medial and lateral hindfoot zones of Type 3 children (p < .05), but their first metatarsal causes higher peak pressures (Table 1).
Table 1 Peak Pressure Registered under the Different Right Foot Zones.
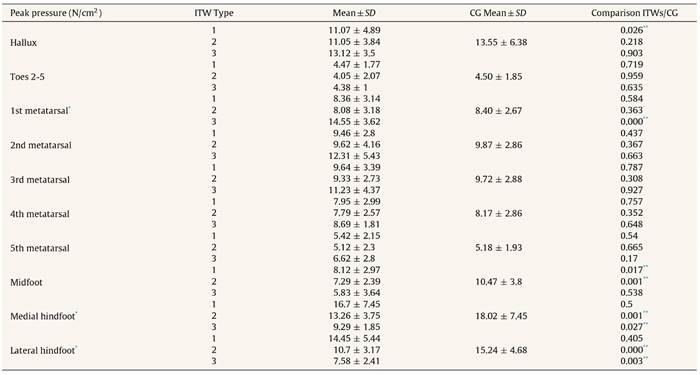
Note. ITWs = idiopathic toe-walkers, CG = control group, SD = standard deviation, N = Newtons.
* p < .05, ANOVA test., differences between ITW types.
** p < .05, Student-t test, differences compared to control group.
Significant differences were found between three ITW types forefoot (p = .005) and hindfoot (p = .012) percentage of impulse. For these zones, all ITW types showed differences (p < .05) with CG in relation with higher impulses exerted by the forefoot and lower by the hindfoot. In addition, total foot impulse was significantly different between the three ITW types (p = .003), with maximum impulse for Type 3 (Table 2).
Table 2 Impulse Percentage Exerted by the Different Right Foot Zones and Total Right Foot Impulse.

Note. ITWs = idiopatic toe-walkers, CG = control group, SD = standard deviation, N = newtons, s = seconds, cm = centimetres.
* p < .05, ANOVA test, differences between ITW types.
** p < .05, Student t-test, differences compared to control group.
Significant differences were found between the three ITW types in contact time percentage of the hallux (p = .001), the second metatarsal (p = .027), and medial and lateral hindfoot (p = .016 and p = .011, respectively). Type 3 ITWs showed a longer forefoot contact together with a shorther hindfoot contact. The analysis of the differences between each ITW type and the CG revealed a specific behavior of the ITW functional unit configured by midfoot and hindfoot, whose contact duration is significative shorther than in CG (p < .05). Conversely, forefoot has a longer contact in all ITW types. Second to fifth toes and first, second, and third metatarsal have a similar behavior in all ITW types (p < .05), but first toe and fourth and fifth metatarsal contact time showed a different behavior between Type 1 and 3 ITW (Table 3). Total step duration was different between types (p = .029), with a progressive longer step from Type 1 to Type 3 ITW and a Type 1 step duration significatively shorter than CG (p = .012).
Table 3 Percentage of Time Contact of the Different Right Foot Zones and Total Step Duration.
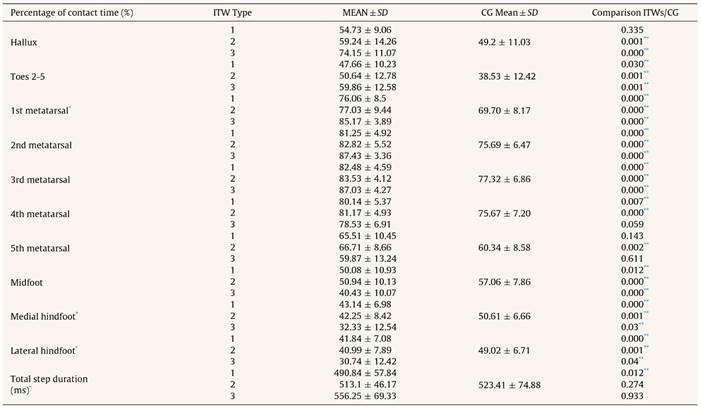
Note. ITWs = idiopathic toe-walkers, CG = control group, SD = standard deviation, ms = milliseconds.
* p < .05, ANOVA test, differences between ITW types.
** p < .05, Student t-test, differences compared to control group.
Orthopedic assessment revealed significant differences between ITW types in ankle dorsiflexion with flexed knee (p = .03), with the lowest passive movement range in Type 3 ITW and differences with the CG in all ITW types (p < .05) (Table 4). With respect to the CG, Type 3 and Type 2 ITW showed a higher pronation angle (p = .049 and p = .031) and Type 2 ITW also demonstrated a higher popliteal angle (p = .021).
Table 4 Orthopedic Assessment of the Right Low Extremity.

Note. ITWs = Idiopathic toe-walkers, CG = control group, SD = standard deviation,° = degrees.
* p < .05, ANOVA test., differences between ITW types.
** p < .05, Student-t test, differences compared to control group.
Neurodevelopmental evaluation by means of CUMANIN revealed significant differences between the three ITW types only for Psychomotricity (p = .047), with Type 2 ITWs showing the lowest development of three types and also in relation with the CG (p = .049) (Table 5). In comparison with the CG, Type 3 ITWs obtained significantly lower farthings in the Memory scale (p = .019), Verbal Development (p = .001), Overall Development (p = .011), and Development Quotient (p = .035). Psychomotricity, Rhytm, and Attention scales and Verbal and Overall Development farthings were the aspects in which ITW children showed the lowest punctuations.
Table 5 CUMANIN Specific Scales and Global Farthings and Development Quotient.

Note. CUMANIN = Cuestionario de Madurez Neuropsicológica Infantil. ITW = idiopathic toe-walkers, CG = control group, SD = standard deviation.
* p < .05, ANOVA test, differences between ITW types.
** p < .05, Student t test, differences compared to control group.
Discussion
All orthopedic and developmental variables in the GC were within normal range for similar population (Engelbert et al., 2011; Hirsch & Wagner, 2004; Portellano, 2004; Portellano et al., 2000; Shulman et al., 1997; Stricker, 2006). Pedobarographical values could not be shared with studies with the same analysis system, but appear to be similar to other studies (Alvarez et al., 2008; Bertsch et al., 2004; Bosch et al., 2010; Liu et al., 2004).
This study demonstrated that the ITW pedobarographic pattern includes a great variability, as some authors have described by means of other gait analysis systems (Alvarez et al., 2007; Crenna et al., 2005). Variability in first foot contact, objetivated through the different zones foot contact beginning, conducted to defining three types of ITW (Figure 1). Similar three pedobarographics models of step development have also been found by some authors in toddlers (Bertsch et al., 2004; Hallemans, D’Aôut, Clercq, & Aerts, 2003; Hallemans et al., 2006). These inicial contact models were related to the functional and morphological foot development, which includes load displacement from the midfoot to the hindfoot and the forefoot and the progressive longitudinal arch development until 6 years of age (Bosch et al., 2010). These three step models have demonstrated to be transitory and evolutionary to the maturation pattern, that some authors situate around the 3-year old age, although gait continues in evolution until the 8 years of age (Fox et al., 2006). Some studies have shown the presence of a first hindfoot roller from the first stages of independent gait, but this does not become a consistent pattern if stability is not acquired. So, heel strike appears when child balance improves (Bertsch et al., 2004; Bosch et al., 2010; Hallemans et al., 2003; Hallemans et al., 2006).
Although we have not found pedobarographic studies in ITW, similar initial contact models have been demonstrated in older ITWs by means of kinetic and kinematic gait analysis by Alvarez et al. (2007). They proposed a gait pattern classification to estabilish its severity and the therapeutical indication, which has been used by other authors to select the most appropriate treatment option and to evaluate its effectiveness (Alvarez et al., 2007; Engström et al., 2010). The similarity of these models with our model and also with inmature ones, as described above, supports the hypotesis about tiptoe gait being considered a specific gait pattern or a sign of neuromotor immaturity, resulting from primitive muscular synergies (Crenna et al., 2005). Tiptoe gait could be considered as physiological in precocious gait stages, in relation with a forward centre of gravity displacement, but this can doubtly be considered and tiptoe gait must always dissapear before being 3 years old (Fox et al., 2006). For this reason, ITW is mostly considered as an abnormal pattern in children older than 3 and its evaluation is strongly reccomended (Alvarez et al., 2007). Pedobarographic analysis appears to be a good clinical and research resource to assess step development in these children.
Pedobarographic gait analysis of three ITW models of step development revealed statistically significant differences between the three ITW types for several variables corresponding with plantar pressure distribution and temporal step development, for all foot zones (Figure 1). Specific pedobarographic, orthopedic and developmental characteristics of each ITW type were also more evident through comparison with the CG (Tables 1-5).
Type 1 ITW, who always heel strikes, showed a plantar pressure distribution model similar to GC one but with midfoot peak pressure significantly lower (Table 1), demonstrating the age-adequated longitudinal arch configuration (Hallemans et al., 2003; Hallemans et al., 2006). Their step development was significantly faster with a forefoot impulse displacement (Tables 2 and 3), in possible relationship with a higher longitudinal axis instability (Hallemans et al., 2003) that causes a fast center of gravity forward displacement (Hallemans et al., 2006), not studied in the present work. These children showed a lower percentage of hindfoot contact time (Table 3), referred in literature as an expression of balance problems in toddlers, and associated with a higher forefoot contact time. Forefoot seems to be able to compensate by muscular control the instabilities from midfoot and hindfoot, more rigid areas (Hallemans et al., 2003; Hallemans et al., 2006). A similar initial contact model was shown by Type 1 ITW from Alvarez et al.’s work, qualified as light ITW (Alvarez et al., 2007).
Type 2 ITW showed a pedobarografic pattern caracterized by significantly lower hindfoot peak pressure and similar in other zones (Table 1). It demonstrated occasional heel strikes but a preferently flatfoot contact, similar to Type 2 defined by Alvarez et al. (2007). This allows a more uniform plantar pressure distribution, that could be considered as a strategy to maintain balance in an instability situation, as described in toddlers (Bosch et al., 2010; Hallemans et al., 2003). In this type the step duration was not significantly faster than CG's one (Table 3).
Type 3 ITW of the present sample, with a retrogradous hindfoot contact, showed significantly higher forefoot peak pressure (Table 1), with a plantar pressure distribution model similar to that found in cerebral palsy children (Femery, Moretto, Renaut, Thévenon, & Lensel, 2002). These ITW generated the maximum forefoot peak pressure of all types, also higher than their hindfoot peak pressures, demonstrating an anteroposterior inversion of plantar pressure distribution with respect to CG and the literature (Alvarez et al., 2008; Bertsch et al., 2004; Bosch et al., 2010; Liu et al., 2004). Forefoot exerted relative impulses higher than 80% (Table 2) and it could be considered as a zone mainly related with gait patern alteration, in a similar way that occurs in cerebral palsy (Femery et al., 2002). Although step duration was not significantly higher than CG's, metatarsals showed a long contact time, longer than 89% of the step duration (Table 3). Alvarez et al. (2008) considered Type 3 ITWs as severe ones, but they did not describe in these children the retrogradous hindfoot contact that we have found (Alvarez et al., 2007), not referred in literature to our knowledge.
As a whole, the comparison between three ITW types and CG revealed that Type 1 ITWs showed a fast step with a forward/anterior load displacement, Type 2 ITWs demonstrated a minor hindfoot use, and Type 3 ITWs did a preferently forefoot gait. From a biomechanical perspective, these gait patterns could represent progressive degrees of the pedobarographic pattern that results from the premature and maintained triceps surae activity during the first half of the support phase. This activity is characteristic of ITW and it is even maintained when they do a spontaneous heel strike gait (Brunt et al., 2004; Crenna et al., 2005). This fact implies a fast center of gravity transition from heel to metatarsal, which appears as gait “by jumping”, usually referred by some parents. It also generates a fast center of gravity forward displacement with a low member movement coordination and muscular modulation alteration that requires precise postural adjustments controlled by the central nervous system. Coordination alteration, with its consequent energetic waste increment and balance maintaining difficulties, could explain frequent falls suffered by ITWs. In these children, clumsiness and exaggerate fatigue caused by physical activities are current problems (Alvarez et al., 2007; Fox et al., 2006).
Orthopedic and developmental assessment of the three ITW types described in this study are strongly related with pedobarographic findings, also showing different severity levels in ITW types classified by their model of step development. Type 1 ITWs only showed a significantly lower ankle dorsiflexion knee-flexed with respect to the CG, whereas Types 2 and 3 ITWs demonstrated a higher foot pronation. Pronation has been referred as a sign of balance difficulties as seen in toddlers with a flatfoot contact at the begining of independent walking (Bertsch et al., 2004; Hallemans et al., 2003; Hallemans et al., 2006) and has been related to triceps-surae length limitation (McMulkin et al., 2006). In ITW, a direct relationship between passive ankle dorsiflexion and ankle movement during gait has not been found (Alvarez et al., 2007; Crenna et al., 2005; Engström et al., 2010; Stott, Walt, Lobb, Reynolds, & Nicol, 2004). However, in our sample, Type 3 ITWs showed dorsiflexion values within normality ranges but significantly lower than other ITW types in the knee-flexed position and also lower than CG in the extended-knee position. This implies the soleus and also the gastrocnemious relation with gait pattern (Table 4) (Crenna et al., 2005). Alvarez et al. (2007) found a dorsiflexion lower than 90° in their Type 3 ITW, lower than in another ITW types and outside normality ranges. This could be an fundamental factor for the lack of heel strike in these children. Nevertheless, in Type 3 ITWs of the present sample a pathological retraction was not found, possibly related to their younger age (Engelbert et al., 2011; Engström & Tedroff, 2012). In this way, gastrosoleus elasticity, together with a higher weight of these children, could have conducted to a retrogradous heel strike before foot switch off (Engelbert et al., 2011). But the minimal number of ITW classified in this type does not let us draw definitive conclusions.
Developmental assessment only demonstrated significant differences between the three ITW types in Psycomotricity (Table 5), but the comparison with CG showed progressive developmental difficulties in relation to the pedobarographic model of step development. Type 1 ITWs did not show differences with respect to CG, but Type 2 ITWs obtained a significantly lower farthing in Pyscomotricity, that could explain the balance difficulties found during gait in these children. Type 3 reached lower farthings in Psychomotricity, Memory, Verbal Development, Overall Development, and Developmental Quotient, demonstrating an inferior neurodevelopment with difficulties also found by other authors in ITW (Shulman et al., 1997; Williams, Tinley, Curtin, Wakefield et al., 2013). These results support the hypotesis about the consideration of tiptoe gait as a sign of a global neurodevelopmental alteration (Shulman et al., 1997; Williams, Tinley, Curtin, Wakefield et al., 2013; Williams et al., 2014).
The gait pattern of the ITWs of the present study is compatible with immature models of step development with a transitory character, expression of a psychomotor delay, or with a permanent character, because of a gait pattern organization alteration (Shulman et al., 1997; Williams et al., 2014). This pattern has some characteristics similar, though lighter, to the cerebral palsy's (Femery et al., 2002), what has been considered as a expression of a minimal cerebral dysfunction (Shulman et al., 1997; Stricker, 2006), also in relation with multisensory integration problems (Williams, Tinley, Curtin, Wakefield et al., 2013; Williams et al., 2014). Its consideration as an inmature pattern is supported by the findings in the ITWs of this study of an initial foot contact similar to that found in toddlers but with a plantar pressure distribution compatible with a structural foot development appropriate for the chronological age, with a progressive configuration of the longitudinal arch (Alvarez et al., 2008; Bertsch et al., 2004; Bosch et al., 2010; Hallemans et al., 2006).
Treatmens are always referred to improve ankle dorsiflexion, usually once retraction has been stablished and there is preliminary evidence for the beneficial effects of serial casting and surgery, but normalization does not seem to occur (van Kuijk, Kosters, Vugts, & Geurts, 2014). However, early treatments that prevent dorsiflexion and gait limitations by dealing with global difficulties of these children have been rarely proposed and their effectiveness have not been yet proved (van Kuijk et al., 2014; Williams et al., 2014).
Pedobarographic classification by ITW models of step development appears to indicate progressive severity levels, in concordance with literature (Alvarez et al., 2007). As these models are linked with specific orthopedic and developmental characteristics, they allow us to propose a specifical therapeutic approach for each ITW type. Type 1 ITW characteristics conduct to indicate for these children a follow-up program with periodical evaluations every 3-6 months, as literature reccomends for ITWs of this age range (Alvarez et al., 2007; Eiff et al., 2006). From an early intervention perspective, this follow-up program could let us evaluate the possible transitory or permanent character of the gait pattern and the development of alterations or compensations with orthopedic risks, aiming at an early treatment to avoid their evolution and structuration (Engelbert et al., 2011; Engström & Tedroff, 2012). Pychomotor difficulties of Type 2 indicate for these children, in addition to the follow-up program, the requirement of a specific therapeutical intervention aimed to enhance their psychomotor development (Alvarez et al., 2007; Eiff et al., 2006). Type 3 ITW requires an inmediate conservative treatment (Alvarez et al., 2007; van Kuijk et al., 2014) because of their mandatory step development pattern with probable effects on foot configuration, ankle range of motion, and upper segments (Engelbert et al., 2011; McMulkin et al., 2006; Shulman et al., 1997; Stott et al., 2004). Moreover, developmental difficulties of this type suggest the possible usefulness of a global and interdisciplinary therapeutical approach considering all the compromised aspects, including the sensorial and the cognitive ones (Shulman et al., 1997; Williams et al., 2014). The Neurocognitive Therapeutic Exercise could be an adequate approach for these children (Martín, Ballestero, & Atín, 2009), but so far this treatment modality has demonstrated scientific evidence only in adults (Cappellino et al., 2012; Marzetti et al., 2014; Zangrando et al., 2014).
Among the limitations of this study, we need to emphasize the restricted age range of the sample, from the age when tiptoe-walking evaluation is recommended to the age when the main foot structural changes have been completed (Alvarez et al., 2007; Bosch et al., 2010). This age range was motivated by the aim of precociously ITW classification and possible alterations prevention. In the baropodometric evaluation, the Hawthorne effect could have influenced the results because of the assessor presence and the great variability of the ITW gait (Eiff et al., 2006; Hirsch & Wagner, 2004; Stott et al., 2004). In addition to that, we have not found children normal values of the studied variables measured up with Footscan® nor their reliability. To minimize the possible influence of these factors, we have analyzed a wide sample, using 10 average records and the foot automatic division in zones (Bertsch et al., 2004). A verification of these models and the estimation of their transitory or permanent character in relation with orthopedic and developmental problems should be confirmed by a prospective study in a wider sample.
Conclusions
Three different models of step development have been described in ITW based on their initial foot contact in a pedobarographic gait analysis. These models have allowed us to classify ITW in three types with progressive severity levels and different orthopedic and developmental characteristics, which suggest the indication of a different therapeutical approach for each of them. The present study confirms that pedobarographic gait analysis facilitates the objective assessing of ITW to clarify therapeutical indications and could also facilitate the evaluation of the effectiveness of different modalities of treatment.

