










 Custom services
Custom services
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
The relatively recent clinical focus of Hospital Pharmacists towards the Emergency Department1-2 has provided opportunities for improvement in the quality, safety and efficacy of patient care3-12.
The American Society of Health-System Pharmacists (ASHP) has defined the Pharmacy services portfolio in the Emergency Unit, and the guidelines that determine the functions of Pharmacists in this hospital department13,14. In 2006, the Pharmacy Care in Emergencies (RedFastER) group was created within the Spanish Society of Hospital Pharmacy (SEFH)15. Its objectives include the improvement in patient care quality through the rational use of medications, and collaboration in patient care, teaching and research with other healthcare professionals and scientific societies. The Australian Society of Hospital Pharmacists has recently published their standards of practice16.
As a result of the coordination between RedFastER and the Spanish Society of Emergency Medicine (SEMES) the consensus document about Medication Reconciliation in Emergency Units17 aims to prevent and decrease medication errors as a shared responsibility among healthcare professionals.
A recent report by the SEFH shows that there is still a limited presence of Pharmacists in Hospital Emergency Departments18. This is a striking fact, because these are clinical units that represent complex settings with a high risk of adverse events: 12%, according to the EVADUR study19, and 24% of them are drug-related errors, near 70% preventables.
Unlike other hospital units, medications are prescribed, dispensed and administered in situ, with a high prevalence of verbal orders, high-risk intravenous medication use in emergencies, high care pressure, and out-patients are managed in a short period of time.
These aspects increase the risk of incidents, and make it difficult to validate medication “remotely”; these are aspects where the Pharmacist can be involved for improving the quality and safety of patient care. Different authors highlight their acknowledgment as members of the Emergency team20,21,22.
The objective of this article is to determine the perception and assessment of Pharmacists by the medical and nursing staff in our hospitals.
Methods
A descriptive multicenter study based on a survey targeted to the members of the Emergency staff, physicians and nurses, from hospitals with a reference pharmacist.
The survey design was based on the survey by Fairbanks and cols.20, validated by its authors.
Some additional questions have been included regarding the characteristics of the hospital, the Emergency Department and physicians, and pharmacist activity:
Teaching accreditation, private or public management, and number of hospital beds
Annual number of patients managed in Emergencies
Medical specialty, if any
Medication reconciliation
The following have been excluded:
Resuscitations and sedations involvement are not part of the clinical activities by Hospital Pharmacists in Spain.
Participation of residents in the survey, because medical training in Emergencies is not acknowledged as a MIR specialty.
The Surveymonkey® tool has been used as electronic
support.
The anonymous questionnaire has an estimated completion time of 10-15 minutes, and includes 14 sections classified into:
Characteristics of survey participants and their institution. It includes dichotomous closed-ended questions (yes/no), multiple choice questions to select one option, and only medical specialty is open-ended.
Perception of the Pharmacist activities in Emergencies regarding patient safety, in three subgroups of questions with closed-ended answer selection, exclusive in the first (only the most relevant activity), and one or more for the two remaining subgroups.
Assessment of the role of the Pharmacist, with two subgroups of seven questions with multiple answers and five possible options for each, according to the Likert Scale (1 = strongly agree, 5 = strongly disagree).
The link was sent to the SEFH mailing list. An explanatory test stated that the Emergency Pharmacist participants had to target the survey to this Unit staff, and confirm by e-mail its potential forwarding. In our hospital, the link and the relevant text were also sent in the same way.
Descriptive statistics were used for the analysis of results, presented through counts, percentages, and their corresponding 95% confidence intervals.
The “strongly agree” and “agree” answers have been summed up and grouped in one single category, as well as the “disagree” and “strongly disagree” answers.
Results
The survey link was sent to the SEFH members on April 15th 2016, and again one month afterwards. Access was available until June 30th 2016.
In our hospital, the survey was conducted earlier. The intention was to obtain the answers under the conditions in which the form had been designed, before the change in the management and structure of the Emergency Dept. Data were analyzed jointly for all participant hospitals.
In total, 835 surveys were sent, and 102 were completed (12%). One survey was considered invalid and discarded.
The Emergency Pharmacists from 20 hospitals confirmed their participations. By region, the participation was: Andalucía (2 hospitales), Aragón (2), Baleares (3), Canarias (1), Castilla-León (2), Cataluña (1), Galicia (1), Madrid (4), País Vasco (1), Valencia (2), Principado de Andorra (1).
A 72% of participants were physicians; 64% of the respondents were female, and 89% have over five years of experience in Emergencies (Table 1).

Fifty-eight physicians stated their specialty: 35 (47.9%) Family and Community Medicine specialists, 18 (24.7%) Internal Medicine Specialists, three Geriatricians, one Intensive Medicine Specialist, and one Occupational Medicine Specialist; five respondents considered themselves “Emergency Specialists”, and the rest gave no answer.
Working centres were mostly public general hospitals, with post-graduate teaching accreditation.
Out of the participants, 81.3% stated working in Emergency Units with high care pressure, > 100,000 visits per year. Participants in hospitals with > 500 beds represented 42.2% of the sample.
Table 2 shows the perception by Emergency staff of the pharmacist activities associated with patient safety.
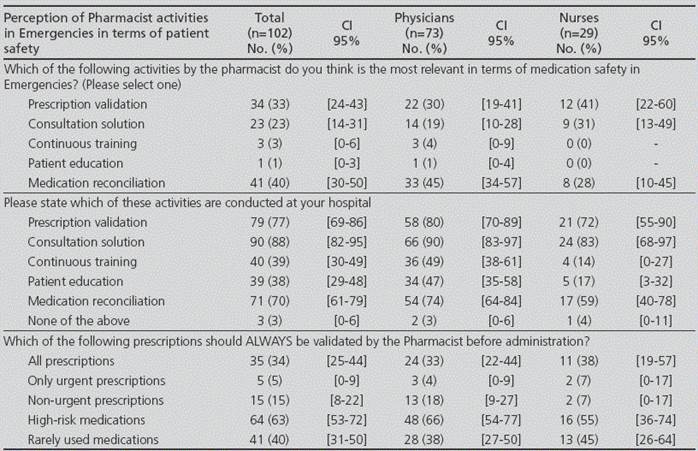
It was considered that the most relevant activities regarding safety were: medication reconciliation (40%), prescription validation (33%) and solution to consultations (23%). No differences were demonstrated by type of respondent.
The following activities conducted were valued: consultation solutions, according to 88% of participants, followed by prescription validation and medication reconciliation, with 77% and 70%, respectively.
Physicians perceived, to a higher extent than nurses, the continuous training by healthcare staff and the information provided to patients by pharmacists in the Emergency Department.
Three participants stated their lack of knowledge regarding these activities being developed in their department.
Regarding treatment validation, 63% of participants considered as a priority that pharmacists should always validate high-risk medications before administration, and 40% for those less used. 34% of participants thought that the Pharmacist should validate all prescriptions previously. Statistical significance is not reached.
Table 3 shows that the Pharmacist improves care quality according to 89% of participants; 87% felt that safety was provided through prescription validation. They were considered useful for healthcare staff and patient training by 81% and 73%, respectively, and as an integral member of the Emergencies team by 77%.

Their actual presence made it easier for professionals to resort to their services, particularly in the case of physicians (84% vs. 52%).
Regarding their usefulness for treatment optimization (Table 4), physicians and nurses highlighted, in this order: information about interactions, dosing adjustment according to the clinical parameters of each patient, and selection of medications based on efficiency criteria (92%, 91% and 77%), while 53% pointed at selection of antimicrobial agents.
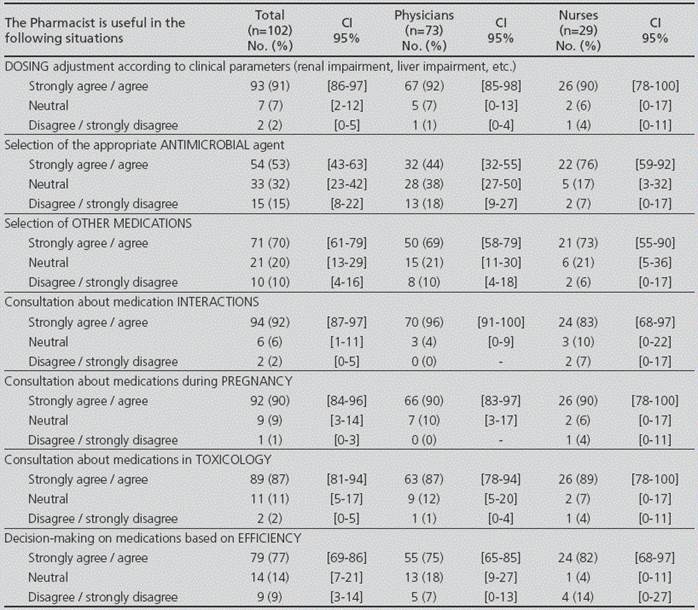
The information provided about the use of medications in specific situations, such as pregnancy or poisoning, was considered relevant by 90% and 87% of participants, respectively.
Discussion
The results obtained showed a positive perception of the Pharmacist by Emergencies professionals, who considered them as integral part of the multidisciplinary team, providing safety and improving patient care quality.
Data reinforced medication reconciliation and prescription validation as useful safety activities.
In the transition between levels of care, 34% of medication errors are clinically relevant and affect 45% of cases23. The Emergency Department is a setting with a high risk of discrepancies and reconciliation errors, both at patient admission and discharge. Therefore, it is recommended that reconciliation takes place at both transition points. Its perception acknowledges the involvement by the Pharmacist in direct patient care.
Likewise, the importance of prospective validation of treatments is highlighted in our study, particularly in terms of high-risk medication, and drugs with less experience of use, consistent with the commitment by Emergencies to safety. It must be pointed out that a third of participants considered that all prescriptions should be validated before drug administration. However, this approach would be difficult, because it would clash with the acceptable delay and therefore, with patient safety.
The participation of Pharmacists in the multidisciplinary team and access to patient encourages their involvement in decisions about treatment in Emergencies.
Unlike previous studies, of which none was located in our setting, decision-making based on clinical efficacy is valued over that based on economic reasons, as well as the optimization of treatments adjusted to the clinical situation of the patient, and the information for an adequate use. The economic impact of those medications more frequently prescribed might not be taken into account in daily practice: this does not only involve the Emergency Unit, but also the next level of care after patient discharge. Undoubtedly, the optimization of costs is one of the tasks of the Emergency Pharmacists.
Only half of the sample considered that Pharmacist intervention was useful for antimicrobial agent selection. This assessment could be explained by the increasingly widespread presence of Infectious Disease Units and Antimicrobial Optimization Programs (PROA), to which Pharmacists have gradually been incorporated.
The lack of knowledge by some survey participants regarding the activities developed could be justified by staff rotation and the Pharmacist / Emergency staff proportion, which is unfavourable to the first one.
The number of answers to the statements “I will contact a Pharmacist more when he is present at the Emergency Dept. vs. when I need to call the Pharmacy Dept.” and “Or I would contact more frequently Pharmacists if they were present at the Emergency Dept.” indicates that these have not been interpreted as mutually exclusive, but as representative of two potential situations at different moments.
The results obtained support the location of the Hospital Pharmacist in the Emergency Unit; they would be more frequently consulted if present, mostly by medical staff. Specifically, medication reconciliation and patient information and education must be developed in situ.
Two studies have been recently published in the U.S.A.24 and Canada25, based on surveys to Emergency Pharmacists; the second study contained specific surveys for the Heads of the Emergency and Pharmacy Departments, respectively. The results obtained in the first study24 showed that Pharmacists spend most of their time conducting clinical activities, such as treatment optimization and follow-up according to the clinical parameters and characteristics of patients, recommendations regarding poisoning cases, training for patients with selected conditions, and medication reconciliation, among others. In the Canadian study25, pharmacists stated that the tasks more frequently conducted were prescription clarification, solution of problems, reconciliation, and dosing adjustments according to renal function. Approximately half of the Emergency specialists considered that the Pharmacist was a valued member of the team.
Both publications completed the information with the time spent and the actual presence of Hospital Pharmacists in Emergencies.
Our study has not considered the time of daily presence or regular location in the unit, which represents a limitation.
The 2015 Report on the Situation of Hospital Pharmacy Units in Spain: infrastructure, resources and activity showed the limited presence of Pharmacists at Hospital Emergency Units18:
In one out of five Pharmacy Units there is a Pharmacist collaborating with Emergencies.
In one out of four hospitals with > 500 beds, the Pharmacist is integrated in Emergencies; and in one out of three, they conduct clinical activity (pharmaceutical care).
In U.S.A., a national survey reported that a Pharmacist was assigned to Emergencies in 6.8% of hospitals in 200826. In 2013, the majority of patients were managed by these professionals in 16.4% of hospitals27. In 2015, around 80% of the Pharmacy Units with activity in Emergencies had a satellite pharmacy24.
The differences in terms of management models and number of pharmacists in Emergencies between these countries are not an explanation for the reduced number of answers obtained in the present study. By hospitals, there is a 6% participation of the total 323 in the public network28, very far from the number of centres with an Emergency Pharmacist18. There is no agreement about what should be considered an acceptable percentage of completion, though some authors report from 50 to 75%29. Anyway, there has been a reduced participation, and there are no differences demonstrated between the nursing and the physician staff in most sections of this survey.
The form of communication used could also represent a limitation, for example if the available e-mail addressed had not been recently updated.
In our hospital, during the course of the study, there was a change in the management and structure of the Emergency Department, and an internal mobility process of nurses was solved; this could have had a negative impact on the number of participants.
The results of this study show the acceptance of Pharmacist by the Emergency staff, who know and value the functions conducted, and highlight the importance of their visible presence. However, new studies are required to assess health outcomes in our setting, and the saving in costs generated by the activity of the Emergency Pharmacist, with the aim to reinforce their widespread presence in the unit.

