










 Custom services
Custom services
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Handling the so-called Hazardous Drugs (HDs) can entail risks for the health of workers, if not conducted adequately.
The term HD was used for the first time in the 90s by the American Society of Hospital Pharmacists1. and subsequently adopted by the American National Institute of Occupational Safety and Health (NIOSH) in 20042 which considers as such all those drugs that show in clinical trials with animals or humans one or more of the following characteristics:
Theratogenicity or other toxicity for development
Reproductive toxicity
Organ toxicity at low doses
Genotoxicity
Drugs with toxicity structure or profiles that are similar to other existing drugs considered hazardous.
Bibliography shows that occupational exposure to HDs can lead to acute or chronic adverse effects (rash, reproductive disorders, or potential chromosomal alterations)3-6. The effects mentioned are considered stochastic: there is a certain likelihood that they will appear, but this won’t necessarily happen. It is very difficult to determine a direct cause-effect relationship between exposure to these drugs and the development of neoplasia or other harmful effects, due to the multifactorial nature of this type of pathological processes. In addition, there is lack of adequate diagnostic or prognostic biomarkers. Faced with this circumstance, the prudence criterion advises to follow the ALARA principle7 (As Low As Reasonably Achievable) regarding exposure to HDs.
At national level, HD handling has been extensively covered in our legislation. Thus, there are a series of mandatory Acts and Royal Decrees that standardize and regulate their handling: Act 31/1995, of November, 8th, on Prevention of Occupational Risks8; RD 773/1997, of May, 30th, on minimum safety and health concerning the use by workers of personal protective equipment9; and RD 665/1997 on workers’ protection against risk of exposure to carcinogenic agents10. The Instituto de Seguridad e Higiene en el Trabajo (National Institute for Safety and Health at Work) has recently published the Technical Information Paper 87.1:16. Hazardous Drugs: Prevention measures for their preparation and administration11.
It is clear and generally accepted that HD handling must be conducted in a centralized manner at the Hospital Pharmacy Departments (PhDs), applying those collective and individual protection measures that are required and recommended by the main scientific societies and current legislation12-17.
The presence of HDs, specifically cytostatic agents, in the healthcare work setting has been demonstrated in multiple international studies18-23, both European and American. In our country, there are currently very few experiences of this type24, but it seems demonstrated that occupational exposure to HDs is a reality, and there is a high likelihood of contact by the healthcare staff, if no precautions are taken.
The main objective of the present study is to assess the presence of HDs in the workplace surfaces of the Compounding Areas at Hospital PhDs in Spain. Secondary objectives include: to quantify the existing quantity (ng/m2) of the HDs analyzed in the workplace surfaces tested, to compare contamination levels (ng/m2) based on the type of surface tested in order to determine potential working areas with a tendency towards HD build-up, and to compare contamination levels between participating hospitals. Likewise, it is intended to evaluate any potential association between the HD levels present and different variables: number of preparations compounded, use of closed drug transfer systems, periodical decontamination processes.
Methods
An observational, prospective, multicenter and transversal study was designed for measuring HD (cytostatic) levels at the compounding areas from the PhDs of ten Spanish hospitals.
Ten hospitals were selected for the sample, preferably with >700 beds, and with centralized HD preparation at their PhD.
The drugs selected to be tested were cyclophosphamide (CYC), ifosfamide (IFO) and 5-fluorouracil (5FU); these were considered surrogate markers for chemical contamination. This selection was conducted due to the specific characteristics of these drugs and specialties (CYC and IFO require previous reconstitution before use, with the subsequent increase in the handling required, and the risk entailed), due to their frequency of use, and the significant amounts that are typically handled.
It was determined that HDs would be handled in the participating PhDs according to their current normalized work procedures. Area and leak cleaning protocols would be applied in the usual manner. Such procedures would be collected and analyzed in order to facilitate the interpretation of results.
Samples were collected by a person designed by each centre, using a sampling kit (CYTO WIPE KIT®) from an independent lab in charge of the analysis and quantifying of the medications tested in the samples (Exposure Control, Sweden AB). The detection limits by the techniques used for quantifying CYC, IFO and 5FU were 0.1 ng/mL, 0.1 ng/mL and 1 ng/mL, respectively. A 100% recovery level was assumed in the samples.
The sample collection procedure was specified in the study protocol. A training video was prepared, explaining the sampling methodology in practice; this video was sent to the centres involved in order to standardize and unify sample collection. For discontinuous surfaces, and due to the difficulty to calculate the surface sampled, a fictional surface was determined as if it was continuous. At the same time, a check list was designed in order to allow the follow-up and record of adequate sample collection by an external observer. This list was sent to the study coordinator at the end of the procedure.
Sample collection was conducted in all centres on October, 26th, 2016, at the end of the working day, before the usual cleaning and/or decontamination procedures, and without previous awareness by workers, in order to avoid any modification in work patterns.
Each centre defined their sample points, with 30 as maximum, and ensured that the following locations were tested:
All biological safety cabinets used for HD handling. In each cabinet: the central workplace surface, front wall, protecting glass by its inner face, air vent closer to the worker, and floor in front of the cabinet.
In the anteroom: The bench where the starting materials are prepared, the bench where final products are reviewed, the external surface of a CYC vial, a 5FU vial and an IFO vial.
In those centres using sterile drapes to cover the central preparation area, said drapes must be sent as one more sample, specifying their surface.
Sample collection was adapted so that the surfaces tested were as comparable as possible with one another.
The centres recorded systematically any incidents associated with handling (leaks, broken containers or vials, etc.) that had occurred during the week before sample collection, and gathered a series of data regarding cleaning and/or decontamination policies, the drug transfer system used, and the number of compounds prepared.
For the purpose of statistical analysis, it was considered that the centre was conducting a decontamination process if there was specific mention of the use of alkaline detergents and/or solutions (NaOH), regardless of its frequency. Those cleaning or disinfection procedures using detergents (without stating their specific alkalinity) or 70% alcohol were not considered specific decontamination processes.
For the descriptive analysis of results, there was a calculation of the mean, standard deviation, median, and first and third quartile in the case of continuous quantitative variables, as well as absolute and relative frequency in the case of categorical variables. On the other hand, a percentile regression model was conducted, with the purpose of studying the potential association between the level of contamination and the fact of conducting a decontamination process, as well as with the number of daily or annual preparations. Given the likelihood that samples collected in comparable places might be similar, the “Sampling location” variable was added as a variable for random effects in the percentile regression model, with the aim to correct any lack of independence in terms of observations; the “Hospital” variable was also added on.
In order to compare the surface contamination levels (median) between the different participating centres and the different sampling locations, the variability in variables considered was represented as a random effect of the model (Hospital and Sampling Location) for each drug.
Analysis was conducted with the R statistical software (version 3.3.3) and the brms package (version 1.5.1). To simulate the most unfavourable circumstance, negative outcomes (below the detection limit) were assigned the maximum non-detectable value that would exist in the surface sampled.
Results
The total number of locations samples was 204, varying between 14 and 30 per centre. In total, 136.367,48 cm2 were sampled, with a total surface sampled of 6.642 to 22.758 cm2 per centre. Table 1 shows the characteristics of sampling, activity, and procedures analyzed in the participating hospitals.
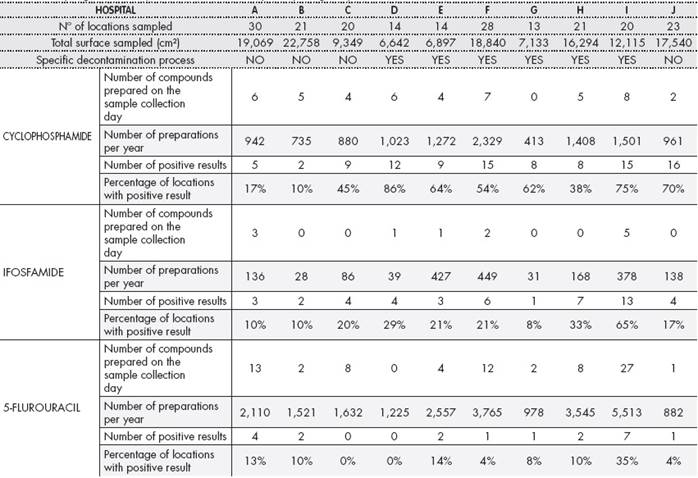
There was evidence of HD present in all centres, with 49% positive samples for CYC (99/204), 23% for IFO (47/204) and 10% for 5FU (20/204). CYC and IFO were present in all participating hospitals, with at least one positive result. Eight centres presented at least one positive result for 5FU (Table 1).
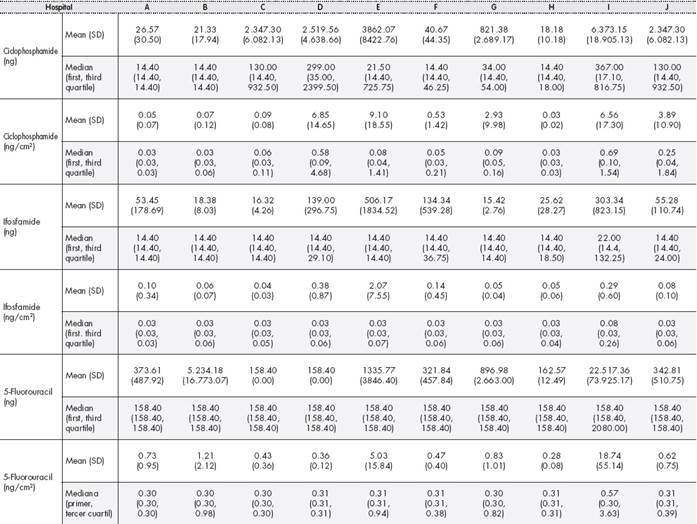
The median (first-third quartile) contamination levels by surface for CYC, IFO and 5FU was 0.05 ng/cm2 (0.03-0.23), 0.03 ng/cm2 (0.03-0.06) and 0.31 ng/cm2 (0.3-0.59) respectively. The mean (SD) and median (first-third quartile) results per center are shown in Table 2.
The statistical model confirmed the existence of significant variability in contamination levels between different centres (for CYC 13.251. CI 95% 7.630 -22.324; for IFO 0.077, CI 95% 0.002 - 0.303; for 5FU 15.027, CI 95% 8.768-25.562); and between different sampling locations (for CYC 0.505. CI 95% 0.011-2.192; for IFO: 0.666. CI 95% 0.418- 1.036; for 5FU 0.547. CI 95% 0.017-1.564). (Figure 1 and Figure 2).


It was observed that the locations with the highest contamination levels were the cabinet air vents. The surfaces sampled with a higher number of positive results were the floor in front of cabinets and their air vents; all centres presented some positive result for at least one of the HDs.
The percentile regression model did not reveal any association between the number of annual preparations for each drug and the contamination levels present in the surfaces sampled for any of the HDs (CYC 1.731. CI 95%-3.617- 17.723; IFO-0.015. CI 95% -0.180 - 0.110; 5FU 4.213. CI 95%-1.288-20.217). Likewise, there was no relationship between the number of compounds prepared on the sampling day and the contamination levels on surfaces (CYC 1.309. CI 95%-11.920-15.015; IFO 0.067. CI 95%-0.105-0.309; 5FU 5.502. CI 95%-5.488-16.170).
Similarly, there was no significant relationship revealed between decontaminating or not the area and the surface contamination levels for any of the drugs sampled (CYC 9.610. CI 95%-5.142-23.349; IFO 0.127. CI 95%-0.051- 0.372; 5FU 5.944. CI 95%-8.030-19.293).
In terms of drug transfer systems, three of the participating centres used a needle isolately for preparation. All centres used a punch with or without vent filter, not classified with an ONB code (FDA). Closed drug transfer systems with ONB classification were not used in any case; therefore, it was not possible to study the potential association between surface contamination levels and the transfer device used.
Discussion
Our study showed the presence of CYC, IFO and 5FU in the PhD compounding areas of all Spanish hospitals analyzed, given that all centres presented at least one positive result for some of the HDs evaluated.
The number of positive results for the total sampled locations was similar for CYC19 to other studies published, but much lower for 5FU24 than those stated in previous studies. This fact can be attributed to the fact that the detection limit in the 5FU quantification technique was 10 times superior to the one for IFO and CYC. Besides, the fact that the vial does not require previous reconstitution reduces the likelihood of exposure. We must add to this the lower volatility presented vs. cyclophosphamide and ifosfamide, which reduces its propagation ability in case of spilling.
In terms of drug amount per surface cm2 contamination levels are low, in comparison with some published studies18 but superior to others20,21,23, where the detection range in some of them is in pg/cm2 a thousand times lower than the one used in this study. This demonstrates the improvement margin existing in our patient care setting.
It must be taken into account that samples were collected before cleaning protocols had taken place, in the same way as for previous studies19: this ensures that results will show the maximum levels of exposure that health-care professionals can be subject to. The comparison with other studies where samples were collected after cleaning23 could be inadequate.
CYC, IFO and 5FU were selected due to previously explained reasons. Moreover, the existing bibliography frequently referred to testing these HDs, which facilitated comparing our results with those for previously published studies. Other studies have evaluated the presence of methotrexate, gemcitabine, doxorubicin and platinum-derivates19,21,23-28 and this is an aspect that should be assessed in future samplings.
The significant variability in contamination levels between participating hospitals shows the need for a deep analysis in future studies of those procedures that might contribute to said variability.
Regarding the study of contamination levels according to the area sampled, similarly to other publications18,27, the places which more frequently presented contamination were the cabinet air vents and the floor in front of them. In our opinion, the presence of HDs in vents is due to the inherent functioning mechanism of the cabinets, and the difficulty to clean adequately non-continuous surfaces. On the other hand, the presence of contamination in the floors brings to light the coordination problems in cleaning and decontamination tasks in workplace surfaces, when different staff groups are involved in said activities (nursing staff, cleaning staff), not always applying the same protocols. This aspect should be analyzed in future studies.
The lack of impact on contamination levels by the number of compounds prepared on the sampling day or annually, suggests that other factors might have an impact on the presence of HDs on workplace surfaces. Other published studies19 showed evidence of the positive relationship between the number of annual compounds prepared and the contamination level: this demonstrates the need to conduct continuous monitoring to confirm or rule out said association in our patient care setting.
The lack of association between contamination levels and the fact of conducting or not a specific decontamination protocol points to the need for specific studies that evaluate this aspect. The heterogeneity between centres in terms of the cleaning and/or decontamination methodologies used, as well as the difficulty to determine which procedures are considered decontamination or mere area cleaning, show the need for developing future studies in order to quantify the effect that one procedure or the other will have on contamination levels.
The main strengths in our study are the high number of participating centres and samples evaluated, as well as the independence of the tests conducted. Besides, it offers an overview of the current situation in Spanish PhDs regarding surface contamination levels.
As main weaknesses, we must highlight the heterogeneity of procedures between the participating centres, as well as its transversal nature, because specific circumstances on the sampling day might have had some impact on results.
We should add that there could be some procedure bias in sample extraction, which was conducted by different persons in each hospital. Likewise, the low detection limit for 5FU could determine the results observed. In other studies, there has been evidence of the influence of the amount of drug handled on the contamination levels on surfaces19, an aspect which was not quantified in our study, and that should be taken into account in the future.
Other aspects that can have an impact on the contamination levels observed and that should be analyzed on subsequent studies are: the facilities available, their maintenance, HD handling protocols, and the use of closed systems, because in our study no hospital was using the latter routinely.
Besides, the fact that this is a transversal study requires confirmation of the results obtained through subsequent samplings, because the conditions in the PhD compounding area can change significantly on specific days. At the same time, the potential incorporation of other centres participating in future studies should increase the strength of results.
As a conclusion, this study brings to light the presence of HDs in the neoplastic compounding areas in Spanish PhDs, the variability between contamination levels in different centres and based on the location sampled. This study opens new lines of research, that will allow to evaluate and improve the results observed. The variability existing between participating centres shows the need to increase the level of standardization of HD handling procedures.
Contribution to scientific literature
There is a limited number of national studies demonstrating surface contamination by Hazardous Drugs in the healthcare setting, and this makes it difficult to establish protection measures for Spanish hospital workers. Besides, the lack of knowledge about the real situation faced will offer a false feeling of safety to those professionals involved and the authorities responsible for establishing applicable rules.
For this reason, it is obviously necessary to understand the real situation regarding surface contamination by Hazardous Drugs in compounding areas at the Spanish Hospital Pharmacy Units. If we are aware of the situation we are facing, we will be able to act accordingly and determine the safety measures required for protecting those healthcare professionals exposed to this type of medications.

