










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Violence against women is a public health problem that cuts across all societies, education and socioeconomic levels, and ethnic and cultural groups (Heise & García-Moreno, 2002). Intimate partner violence (IPV) is one expression of violence against women. In low and middle-income countries of the Americas, IPV prevalence among ever-partnered women is around 30% (2013), and in some countries it reaches 50% (Bott, Guedes, Goodwin, & Mendoza, 2012). In this paper, IPV is defined as any actual, attempted, or threatened physical harm perpetrated by a man against a woman with whom he has, or has had, an intimate, sexual relationship (Kropp & Gibas, 2010).
In the last 20 years, identification of the factors that increase (or decrease) the occurrence of this type of violence has become a primary task in the prevention of violence against women (Capaldi, Knoble, Shortt, & Kim, 2012; Krug et al., 2002). Efforts have also been made to generate empirical evidence on structured techniques that assist professionals in this task (Nicholls, Pritchard, Reeves, & Hilterman, 2013). Tools such as the Spousal Assault Risk Assessment guide (SARA; Kropp, Hart, Webster, & Eaves, 1999), the Brief Spousal Assault Form for the Evaluation of Risk (B-SAFER; Kropp, Hart, & Belfrage, 2005), the Ontario Domestic Assault Risk Assessment (ODARA; Hilton et al., 2004), the Domestic Violence Screening Instrument (DVSI; Williams & Houghton, 2004), and the Danger Assessment (DA; Campbell, 1995; Campbell, Webster, & Glass, 2009), are the IPV risk assessment instruments with the highest empirical contrast around the world (Hanson, Helmus, & Bourgon, 2007; Nicholls et al., 2013). The fundamental difference between them is in the criterion to be predicted. For example, while the SARA and the B-SAFER evaluate the risk of a wide range of new physical violence incidents against an intimate partner of any sex, the ODARA evaluates the risk of violent recidivism against a female domestic partner among men with a police record for such violence, and only the DA has been designed to assess the risk for lethal violence (Otto & Douglas, 2010).
The evaluation of risk factors not only enables an estimate to be made of the risk level of a woman under specific conditions to suffer a new violent event from her partner or ex-partner, but also assists professionals to identify the targets to which they must direct the intervention strategies to reduce risk (Belfrage et al., 2012; Kropp, 2008). This is especially relevant in contexts with limited resources, since the most dangerous batterers can receive services first and receive more intensive monitoring (Cattaneo & Goodman, 2005). Furthermore, IPV risk assessment is suitable not only in police, legal, or correctional services where decisions on aggressors and victims are required daily (López-Ossorio, González Álvarez, Buquerín Pascual, García, & Buela-Casal, 2017), but also in the community health context, due to its central role in the process of IPV detection and intervention (Alvarez López, Brito, Arbach, & Andrés-Pueyo, 2010; Colombini, Mayhew, & Watts, 2008; Messing & Thaller, 2015).
Among Spanish-speaking countries, Spain has led the field in structured IPV risk assessment, with extensive developments in correctional (Echeburúa et al., 2013; Echeburúa, Amor, Loinaz, & de Corral, 2010; Lila, Oliver, Galiana, & Gracia, 2013; Lila, Oliver, Lorenzo, & Catalá, 2013; Loinaz, 2014), forensic (Andrés-Pueyo, Lopez-Ferrer, & Alvarez López, 2008), and police (Garrido-Antón, 2012; López-Ossorio et al., 2017; López-Ossorio, González, & Andrés-Pueyo, 2016; Santos Hermoso & Gonzalez Álvarez, 2017) contexts. Researchers and professionals working on a daily basis in these contexts have been very productive in recent years in systematizing empirical research on IPV risk assessment and management, and this, as from the late 1990s, had a relatively rapid impact on professional practice across many official institutions (Arbach & Andrés-Pueyo, 2016; Arce & Fariña, 2010; Echeburúa, Fernández-Montalvo, & de Corral, 2009; Lila, Oliver, Galiana et al., 2013; López-Ossorio et al., 2017; Muñoz Vicente & López-Ossorio, 2016).
The violence risk assessment perspective was also adopted for community health services by the Barcelona Network Against Gender Violence [Circuit Barcelona contra la Violència vers les Dones, or CIRCUIT in Catalan], in the northeast region of Spain. Between 2008 and 2009, the CIRCUIT developed an instrument to improve professional assessment practices and communication between the many different facilities in the network (e.g., health, police, social, legal, and educational services, including non-governmental organisations). The tool is named RVD-BCN (in Catalan, Risc de Violència vers la Dona-Barcelona), referring to the risk of violence against women (Álvarez et al., 2011).
The RVD-BCN is based on the structured professional judgment model for assessing the risk of severe physical violence by intimate partners. It was designed to be completed when the main source of information is the victim report and no interview with the aggressor is available. There are two versions, the preliminary version used in the original study with 19 risk factors and the final version with 16 risk factors, related to the violent, criminal, and clinical history of the man and some victim vulnerability factors. The RVD-BCN was prospectively validated between 2009 and 2010 in a sample of 216 women attending the CIRCUIT facilities. The instrument demonstrated good levels of internal consistency (α = .71) and predictive validity for the most severe forms of physical violence during a six-month follow-up (with Area Under the ROC-Curves around = .72), suggesting that it may be useful in the assessment and short-term management of this type of violence (Arbach & Andrés-Pueyo, 2014).
In addition to the empirical evidence of its validity, two other features of the instrument make it eligible for being adapted to other contexts. First, both the user manual and the scale itself have been registered under a Creative Commons license, so its free use is permitted (http://goo.gl/kS6rHV). Second, acceptable levels of satisfaction have been reported by users of the instrument (Andrés Pueyo, Arbach, Lopez-Ferrer, & Nguyen-Vo, 2011, p. 215). Nonetheless, there are no studies testing the predictive validity of the tool in other samples.
In Argentina, studies about violence risk assessment have been carried out by specific research groups, which have been prolific in adapting and validating the tools most used around the world for the South American region (Folino, 2015), including those specific for IPV risk assessment (Kropp, Hart, Webster, & Eaves, 2004). However, local institutions have not generalised this technology into their usual professional practice (Arbach, Bondaruk, Carubelli, Palma, & Singh, 2017; Goldstein, Houck, & Folino, 2015; Singh, Condemarín, & Folino, 2013). For example, the national program for IPV prevention and assistance, which has an annual budget of 10 million dollars, makes no mention of structured IPV risk assessment (Consejo Nacional de las Mujeres, 2016). Moreover, despite figures of violence against women that reach 400 femicides and 86,700 reports per year (Instituto Nacional de Estadística y Censos, 2018), and the resulting strength that feminist movements have gained in Argentina in recent years (Goñi, 2016), no research has been found in PsycINFO, Scopus, ISI Web of Science, Google Scholar, or Latindex reporting data on the validation of techniques for structured intimate partner violence risk assessment in this country. Therefore, the main objective of this study was to analyse the predictive validity of the RVD-BCN for IPV in a sample of female users of community health facilities in Cordoba, a city in the central region of the country with 492,000 adult female inhabitants.
Method
Participants
The sample was composed of 321 women who attended five public community health facilities: one general hospital (n = 108), one teaching maternity hospital (n = 73), one state maternity hospital (n = 59), the Provincial Council for Women service (n = 53), and one primary health care centre (n = 28). Average age for the total sample at assessment was 37.14 years old (SD = 13.54, range 18-81). The selection criteria were: being more than 18 years old and having had at least one male partner in their lives. Most participants had a male partner at the time of assessment (73.5%) and reported data about him. The rest of the women reported data on their former partner; 63.5% had at least one child, 58.8% had secondary or higher educational level and 52.7% had a paid job. There were differences in the frequency distribution of these characteristics across institutions (see Table 1).
Table 1 Women Sociodemographic Characteristics: Comparisons between Institutions

Note. A = general hospital (n = 107); B = teaching maternity hospital (n = 72); C = state maternity hospital (n = 58); D = provincial council for women service (n = 53); E = primary health care centre (n = 27).
Significant differences were found in mean age, F(4, 302) = 14.20, p < .001. Post hoc comparisons using the Bonferroni test indicated that the mean age for the Provincial Council for Women service (M = 46.85, SD = 1.30) was significantly higher than the rest of the institutions. In addition, significant differences between institutions were found in women having a partner, χ2(4, N = 317) = 30.89, p < .001; child in charge, χ2(4, N = 315) = 58.00, p < .001; educational level, χ2(4, N = 316) = 48.97, p < .001; and having a paid job, χ2(4, N = 306) = 29.17, p < .001 (Table 1).
Instrument
We used the original research version of the RVD-BCN [in Catalan, Risc de Violència vers la Dona-Barcelona] (Álvarez et al., 2011), which collected information on 19 dynamic and static risk factors, coded dichotomously (0 = absence, 1 = presence) to reach a total score which could range between 0 and 19. After the risk factor information is processed, a final summary risk judgment is required to be made by the assessor that reflects his/her overall professional opinion of IPV risk on a three-point scale (low, moderate, or high) (Andrés Pueyo et al., 2011). This is one of the main characteristics of other instruments based on the structured professional judgment model, such as the Spousal Assault Risk Assessment (Kropp & Gibas, 2010). The predictive validity of this variable was not explored in the original validation study, but a significant correlation was reported with the risk categories established from the ROC curve analysis (r = .56) (Andrés Pueyo et al., 2011, p. 167).
In the original validation study, the mean score of the 16-item version was 7.1 (SD = 2.8) and total scores, which could range between 0 and 16, were significantly correlated with physical violence at three (r = .19) and six (r = .22) months. Furthermore, cut-off scores were established for low (0 to 7, 53% of the sample), medium (8 to 9, 29%) and high (> 10, 18%) IPV risk levels. This categorisation was a good predictor of physical violence in follow-up at 3 (AUC = .77, 95% CI = .68-.87) and 6 (AUC = .80, 95% CI = .71-.90) months, and showed low predictive properties for psychological or minor forms of sexual coercion. Good indexes of inter-rater reliability were also obtained (Andrés Pueyo et al., 2011).
Procedure
The Ethics Review Committee of the Provincial Maternity Hospital and the National Clinical Hospital of Córdoba approved the research protocol and its administration in the five institutions. The risk assessments were conducted between October 1, 2014 and August 1, 2016, in the context of routine professional practice in the five public community health facilities of the city. In all, we trained 40 assessors (one social worker, one nurse, and several psychologists, physicians, and advanced Psychology students). All of them received 4-to-8-hour training according to their time availability.
Participants were recruited during routine interviews by professionals who explained the aims, methodology and implications of their participation, as well as their freedom to refuse or withdraw their participation in the study at any time without any negative consequences for them. If they agreed to participate, an informed consent was required before they proceeded to the semi-structured interview. Assessments were conducted on the basis of the interviews with women and assessors were not required to consult other sources. Following the principles of the structured professional judgment model, we asked assessors to report a summary risk rating in order to compare using numerical scores.
Study Design
This was a prospective multicentre study with a follow-up at a minimum of one month. The calculated follow-up time between the IPV risk assessment and the end of the follow-up period for the current sample ranged from 47 to 311 days (M = 133.70, DS = 49.82). There is complete follow-up data for 230 women (72% of those approached). Follow-up interviews were made personally (n = 28, 12%) or by telephone (n = 202, 88%) between January 22, 2015 and December 19, 2016. During this phase, three women did not appear for the scheduled personal interview and 88 women could not be reached after 10 telephone calls. Thus, the follow-up periods varied according to the availability of the women to respond the interview. The personal interview was made by the same assessor as at base assessment. Telephone assessments were made by trainee advanced psychology undergraduates. Of those women contacted by phone, only 6% refused participation during follow-up. At the beginning of the telephone conversation, instructions were provided to guarantee the safety of the victims during the time the call lasted.
Predicted Outcome
In the follow-up, assessors asked women for information about the occurrence after the baseline assessment of several behavioural indicators of physical and sexual violence perpetrated by the current or ex-intimate partner about whom they reported in the base assessment. These indicators included: slapping, pulling hair, pushing, hitting, beating, dragging, kicking, attempted strangulation or attempted burning, throwing objects to hurt, using a knife, weapon or object to attack, forced sex under threats, intimidation or physical coercion, and finally, threats of physical damage against her or her relatives. If participants were detected as being currently victims of violence, they were contacted by the professional who evaluated them in their reference institution so that they could put appropriate protection interventions into effect.
Statistical Analysis
Descriptive analyses (i.e., mean, standard deviation, range, percentages) were performed to explore the distribution and dispersion of variables. A chi-square test was calculated to analyse the independence between summary risk ratings at the baseline assessment and the outcome variable dichotomised as violence present (1 = any indicator occurring at least once during follow-up) or absent (0 = no indicator during follow up), and also to analyse independence between each risk factor and subsequent violence. RVD summary risk ratings were used as an independent variable in analyses.
Only risk factors with a significant association with an outcome variable in bivariate analyses were added to obtain RVD scores. We did not score the RVD if more than four items had missing data. In consequence, seven cases were considered missing for the total score variable, but not for the item level analysis. Internal consistency analyses were performed, and normal distribution was explored using the Kolmogorov-Smirnov test. A Mann-Whitney test was used to compare the RVD total scores between women who had suffered one or more IPV event during follow-up and those who had not.
Receiver Operating Characteristic (ROC) curve analyses were used to examine the predictive validity of the RVD total score and summary risk ratings to predict IPV. ROC curve analysis is widely used in predictive validity research for violence risk assessment tools (Singh, Desmarais, & Van Dorn, 2013). The ROC curve is a plot of the true and false positive rates for the tool, and the area under the curve (AUC) parameter (range 0-1) can be used to compare accuracy between measures. It is particularly useful, as it provides data that are fairly independent of the base rate of violence in a population (Mossman, 1994). Instruments or clinicians able to distinguish violent from non-violent individuals with nearly perfect accuracy would have ROC-AUCs approaching 1.0, and AUC .50 represents no better than random prediction. In general, ROC-AUCs of .75 are considered large effect sizes (Dolan & Doyle, 2000), but recent recommendations on how to report ROC analysis results have been taken into account (Singh, 2014).
To incorporate the length of time from the day of base assessment until the follow-up assessment, survival analyses were carried out. The time-at-risk taken into account was the total of days between assessments. The dichotomous outcome variable was used in a Kaplan-Meier bivariate survival analysis. Cox regression survival analysis was used to examine whether the RVD summary risk ratings added incrementally to the RVD numerical score. A measure’s incremental validity is its ability to provide significant information to the prediction when an alternate variable has already been entered in the model. In doing so, the RVD scores were first entered in a hierarchical Cox regression at block 1, while the summary risk ratings were entered at block 2, with time-at-risk entered as the time variable, and the dichotomous IPV event as the status.
The statistical significance level used was p < .05. Statistical analyses were performed with the IBM SPSS software version 24.0 (IBM Corp., 2016). The data was entered in an ad hoc database with security measures.
Results
Participant Outcomes
The overall victimisation rate at follow up was 9%, i.e., 21 participants reporting at least one event of IPV by their partner or ex-partner during that period. The most frequent outcome was threats (7.4%), followed by slapping, pulling hair or pushing (4.3%), forced sex (3.9%), hitting or beating (2.2%). The remaining violent behaviours had a prevalence rate of 1.3% each.
Predictive Validity
The summary risk rating estimated at the baseline assessment was significantly associated with the occurrence of violence during follow-up, χ2(2, N = 225) = 68.99, p < .001 (Table 2).
Table 2 RVD Summary Risk Rating and Intimate Partner Violence during Follow-up
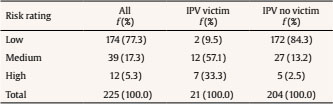
Note. IPV = intimate partner violence.
We conducted an item-level analysis to know if single items had a unique association with IPV victimisation during follow-up (Table 3). Five vulnerability factors were independent of the IPV condition established prospectively. They were therefore removed from subsequent predictive analysis.
Table 3 Rate and Odds Ratio for each RVD Risk Factor and Intimate Partner Violence during Follow-up

**p < .01, ***p < .001.
After removing variables not associated with violence in the bivariate analysis, a total score was calculated with one point for each risk factor present. Cases with four or more items without information were removed to avoid cells with missing data. Initial analyses using the Kolmogorov-Smirnov test suggested that the total RVD scores in the entire sample were not normally distributed, D(315) = 0.28, p < .001. The total mean score for participants who completed the follow-up was 2.54 (SD = 3.27, range 0-14, Mdn = 1) and showed no significant difference with the mean of missing cases (M = 2.62, SD = 3.27, Mdn = 1) (U = 9891.50, p = .697). The reliability of the 14-item scale was moderate to high (α = .85). RVD scores were higher for those women who had suffered one or more IPV event during follow-up (M = 8.55, SD = 4.48, Mdn = 9) compared with those who had not (M = 1.91, SD = 2.44, Mdn = 1), U = 472.5, p < .001.
The total score AUC was .89 (95% CI =.79 to .98, p < .001), while the summary risk rating AUC was .88 (95% CI = .80 to .97, p < .001). This suggests that the probability that a randomly selected victim woman had a higher score or a higher risk rating than a randomly selected non-victim woman was 89% and 88%, respectively. Although there is considerable variability in what constitutes a small, moderate, and large value for AUC (Singh et al., 2013), there is general agreement that this effect size represents good discrimination (Rice & Harris, 2005).
Survival Analyses
Survival analyses take differences in time-at-risk into account and check for unequal follow-up times between participants. Low-risk participants not only suffered fewer events of IPV during follow-up than participants in the moderate- and high-risk groups, but also suffered them later in time. The mean survival time for those participants with high and moderate risk was 157.8 (EE = 30.8) and 175.2 days (EE = 12.5), respectively, versus 287.9 days (EE = 2.9) for participants with a low risk level. The risk groups emerged as significant predictors (log rank = 76.4, df = 2, p < .001) (Figure 1). The mean number of follow-up days did not differ between groups (F = 1.09, p = .34), so differences cannot be attributed to differences in time-at-risk.
Figure 1 shows the rate of IPV events over time for the three summary risk rating groups (low, moderate, high). Log rank tests found significant differences between IPV events of the low risk group (top line) and both the moderate-risk group (middle line), χ2(1) = 51.45, p < .001, and high-risk group (bottom line), χ2(1) = 84.40, p < .001. No significant difference was found between the moderate- and high-risk groups, χ2(1) = 2.20, p = .14.

Incremental Validity
To account for variations in follow-up time and to assess the incremental contribution of summary risk ratings in predicting recidivism with the RVD scores, a hierarchical Cox regression survival analysis was conducted. The RVD total score was entered at block 1, the summary risk ratings variable at block 2, with the time-at-risk entered as the time variable and the dichotomous IPV variable as the status. The summary risk ratings were entered as a categorical variable (low, moderate and high), and as three dummy variables each collapsing two risk categories (i.e., low vs. moderate/high, low/moderate vs. high, and low/high vs. moderate).
A significant block 1 effect was revealed, χ2(1) = 76.04, p < .001, -2LL = 139.26. The summary risk ratings entered as block 2 produced a significant improvement to the model’s fit (χ2 change = 7.61, df = 1, p < .01). The predictive model composed of the RVD scores and the moderate/high vs. low risk variable showed a good adjustment (-2LL = 131.643, χ2 = 79.64, df = 2, p < .001). Thus, this analysis shows that summary risk ratings added incrementally to numerical RVD scores (Table 4).

Discussion
The primary goal of this research was to see if the RVD, an instrument for estimating IPV risk in community health facilities, is applicable to populations in Argentina. Our results show that the accuracy of the prediction of future IPV events was good for an adapted 14-item version of the instrument and closely resembled the prediction efficacy of the original RVD 16-item version, and other risk assessment measures in the context of IPV (Nicholls et al., 2013). Furthermore, results show that the summary risk judgments increase the predictive power of the numerical RVD score. Similar findings have been reported for the SARA (Kropp & Hart, 2000) and give support to the idea that little difference exists between actuarial (statistical) and structured tools in predicting violent reoffending, although this does not suggest they are equally informative for case planning, particularly when the goal is to reduce risk (Campbell, French, & Gendreau, 2009). Therefore, we believe that this study provides a sound evidence base for the use of structured violence risk assessment instruments within community facilities where women attend on a regular basis. Physicians, nurses, social workers, psychologists, and other professionals working across a number of professional settings are likely to encounter individuals experiencing IPV, in part due to its negative physical and mental health consequences (Campbell, 2002a; Messing & Thaller, 2015). Thus, an IPV risk assessment instrument, such as the RVD, could be utilised in safety planning, advocacy and counselling (Campbell, 2002b). As was pointed out in a previous validation study, this does not necessarily mean that these instruments will also be effective in any female population or that other instruments will also be effective in this group (Snowden, Gray, & Taylor, 2010). Clearly, further research is needed to secure a sound evidence base for any specific female population (e.g., adolescent or young, disabled or mentally disordered). However, these results support the converging evidence indicating that the combination of a few out of several possible risk factors can be used to produce an effective prediction instrument and that these factors appear to cross most cultural boundaries (Snowden et al., 2010). Hence, while direct evidence is still needed, it would seem likely that this instrument will be effective in other Latin American countries.
As the literature reveals a shortage of prospective, longitudinal studies (Nicholls et al., 2013), the design of this study is a strength, since the occurrence of violence was registered prospectively, which minimized confirmatory biases in the risk assessment process. Nonetheless, prospective predictive research is hampered by meeting the clinical goals of risk assessment, i.e., risk management and prevention (de Vogel & de Ruiter, 2006; Dernevik, Grann, & Johansson, 2002). Thus, it is very likely that subsequent risk management was influenced by the results of the risk assessment. In our study, professionals were able to use the results of the RVD ratings, for instance, for decisions concerning requests for protection orders or to encourage women to make a police report. High-risk participants were referred to specialised care services where they would receive protection measures. In consequence, a higher RVD risk rating could cause increased surveillance, leading to more effective risk management and treatment and to fewer episodes of violence to observe during follow-up. So, the predictive validity indexes that we obtained were already high and similar to those reported for the original study (Arbach & Andrés-Pueyo, 2014), but might have been even higher if the results had not already been used to manage risk.
Previous findings support the belief that appropriately structured risk assessment can prevent violence by informing risk management decisions (Belfrage et al., 2012; López-Ossorio et al., 2017). Thus, as a fruitful line of research in our region, we propose the systematic study of the preventive efficacy that can be obtained by matching the RVD assessment results with the available resources.
The RVD has proven to be a useful tool for the evaluation and management of short-term risk. This is a strength, considering that the critical period of highest recidivism of aggressors is found within the first six months (López-Ossorio et al., 2017). Whether the instrument is useful beyond that period is an empirical question, and it should be explored in future studies. The same applies to the question of whether our findings would be replicated if other forms of violence were used as a criterion. It must be taken into account that the available evidence indicates that physical violence against a partner can be significantly differentiated from other forms of violence, such as lethal violence, or that they can even be different phenomena (Santos Hermoso & Gonzalez Álvarez, 2017). Therefore, the use of RVD is recommended for assessing the risk of the behaviour for which it was validated, i.e., physical violence.
Despite the novelty of this study in the context in which it was developed, some limitations must be considered when interpreting the results. First, the sample was derived from only one Argentinean adult female community sample, thereby limiting generalisation. Nevertheless, we consider this group to be representative of women of the general population attending community facilities, because they are largely similar in demographic characteristics to the total population of adult women in this city (see Gobierno de Córdoba, 2010).
Second, inter-rater reliability of the tool, i.e., the degree of agreement among raters, remains a subject for future research. The workload of professionals and the limited time in public institutions made it difficult to carry out independent evaluations. Although their training was aimed to reduce any assessors’ biases, it is not possible to know in this study the extent to which the assessments were based on the same clues.
A final limitation is that data regarding violent outcomes may not always be reliable. For example, it is possible that women do not report incidents of physical violence in the telephone follow-up calls due to lack of confidence with the interviewer or to an inadequate environment when answering the phone call. Nonetheless, training and supervision of the interviewers was carried out to minimize this effect, and the value of this methodology for screening sensitive topics has been established elsewhere (Mealer & Jones, 2014). Furthermore, although the base rate of violence was relatively low (9%), regional accounts report figures of IPV victims in the last year prior to the assessment ranging from 8 to 25% in other South American countries (Bott et al., 2012). It should be noted, however, that most of these limitations would have had a negative effect on the predictive accuracy of the RVD, and thus the findings might have been even stronger without these limitations.
Conclusions
The present study is the first evaluation of violence risk assessments completed using the revised version of the RVD, and the first study to include the RVD summary risk ratings in the prediction model. Its findings add essential new information to the growing evidence supporting structured professional judgment as an approach to assess and manage risk for violent outcomes among females attending community health facilities. They also contribute to the emerging practice of including structured violence risk assessment in Latin American professional contexts and institutions (Arbach & Andrés-Pueyo, 2016; Folino, 2015; Goldstein et al., 2015). An important next step will be to examine whether consideration of a predetermined list of risk factors, and the use of RVD in particular, improves risk management efforts and ultimately reduces the prevalence and severity of violent outcomes. Finally, a comprehensive assessment of violence risk should include consideration of other contextual or institutional factors that have been identified as important variables increasing or decreasing the likelihood of IPV (e.g., the resources available for intervention and the knowledge of such resources by professionals) (Colombini et al., 2008). Although there have been some recent efforts in this area (Belfrage et al., 2012), further work is needed, especially in more disadvantaged regions.

