










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Laparoscopic radical prostatectomy (LRP) is considered the standard treatment for clinically localized prostate cancer.
LRP pain is lesser than that of open surgery, but it is still considered as moderate 1. Literature results on the optimal analgesic technique are conflicting 2) (3) (4) (5, with actual guidelines encouraging a multimodal approach 6 to reduce the amount of opioids administered, thus minimizing side effects 2) (7. Several studies have been published, where different analgesic methods are considered: patient-controlled analgesia (PCA) of morphine chloride 2, epidural technique 3, use of drugs for neuropathic pain control 4, or surgical wound infiltration. However, there is no clear consensus on the best analgesic technique for this type of surgery.
The benefits of optimal postoperative analgesia are clear, and include a reduction in the postoperative stress response, which can lead to organ dysfunction and prolong recovery time 8. Appropriate analgesia translates in lesser postoperative morbidity and improved surgical outcomes, accelerating rehabilitation without increasing the number of readmissions or complications 9.
Hence, the usual practice in our hospital is the epidural technique with local anesthetics, which has been considered the most adequate analgesic technique for this type of surgery, as it improves pain control and patient comfort, decreasing secondary effects of other analgesics, and the number of complications 7) (10. However, this technique has certain contraindications and is associated to complications such as numbness or motor weakness 11) (12, requiring close monitoring to ensure its safety and efficacy, not delaying the rehabilitation period. Moreover current practices advocate in favor of a less invasive analgesic therapy, which seems to be sufficient for this kind of surgical approach.
As part of a larger, prospective study comparing the analgesic efficacy of epidural technique vs. TAP technique for PRL pain, we performed this retrospective study of all epidural-controlled LRP performed in our hospital between 2010 and 2015. Our aim was to describe the analgesic quality of this technique, as well as its complications in the postoperative period.
MATERIAL AND METHODS
A retrospective analysis of all patients who underwent LRP for prostate cancer between 2010 and 2015, in which epidural analgesia was the postoperative approach, was performed. This analysis was carried out in the design of a study comparing the epidural technique with another analgesic technique. We performed the analysis of the last 5 years to see the results obtained and to be able to evaluate them with those that will be obtained in the study that is currently in progress. Exclusion criteria included those patients where regional anesthesia was contraindicated (due to patient's rejection or lack of collaboration, bleeding disorders, including heparin use, puncture site infection, allergy to local anesthetics, neurological disorders), and those patients where surgery was reconverted from LRP to open surgery.
Management of patients undergoing LRP
The procedure is generally performed under combined anesthesia, as follows. Under standard monitoring (electrocardiogram, pulse oximetry and noninvasive blood pressure), a peripheral venous access is obtained and intravenous midazolam (1-2 mg) is administered for anxiolysis.
In those patients without contraindications 13, epidural technique with loss of resistance (serum or air) approach is performed at either thoracic or lumbar level, depending on each anesthesiologist's usual practice. A test dose of 3 mL epidural 2 % lidocaine is given.
The patient is transorally intubated, after anesthetic induction is performed with fentanyl (1.5 mcg/kg), propofol (1.5-2 mg/kg) and rocuronium (0.6 mg/kg). Maintenance is performed with sevofluorane (CAM 0.6-1). For analgesic control, an initial epidural bolus of between 6 and 8 mL levobupivacaine 0.25 % is administered, with further hourly bolus of between 5 and 8mL, depending on pain assessment by usual parameters.
After surgery, the patient is extubated and transferred to the postoperative acute care unit (PACU), where he remains for the first 12 hours after surgery, for pain and bleeding control. An infusion of local anesthetic (LA) (levobupivacaine 0.125 % or bupivacaine 0.125 % with or without fentanyl 2 mcg/mL) is begun and maintained at either 5 or 8 mL/h (elastomeric pump reservoir). If motor blockade or hypotension due to vasoplegia is detected, the infusion is suspended until reversal of effects. On the other hand, in case of uncontrolled pain, a bolus of 5 mL 1 % lidocaine is administered, with reposition of epidural catheter if there is no improvement.
It has been demonstrated that postoperative pain control is effective both as PCEA (Patient-controlled epidural analgesia) 14) (15 as in CEI (continuous epidural infusion) 16) (17 mode. As PCEA pumps are not available in our center, CEI was used.
Intravenous postoperative analgesia consists in paracetamol 1 g/8 h ev and dexketoprofen 50 mg/8 h ev. In situations of renal impairment, gastric problems or allergies, metamizol 2 g/8 h ev was administered.
During the post-operative period, the anesthesiologist and the nurse from the acute pain unit (APU) visit the patients daily, evaluating and registering catheter function, pain, and possible complications. Catheter removal is performed when VAS were consistently <3 in patients with low doses of epidural analgesia, without blood coagulation alterations nor low molecular weight heparin (LMWH) administration within the previous 6 hours.
Data Collection
Data was obtained via retrospective review of clinical histories, including the anesthesia sheet, nurse's charts and urology charts, and the APU's registries. From these, data on the epidural technique, drug administration, general evolution and possible complications was obtained.
According to the previous description, the following data was recorded: anthropometric parameters (age, weight, height, ASA); data related to the epidural technique (distance to skin of epidural space, length of catheter inserted) and possible difficulties when performing it (vascular puncture, spinal puncture, impossibility of performance, subdural block); data on epidural infusion (type of LA administered, infusion rate); catheter-related complications (accidental disconnection); postoperative pain data (visual analog scale (VAS) at rest and in movement at PACU, and daily); appearance of neurological side effects (motor block according to the Modified Bromage scale: I: no block: free movement of legs and feet; II: Partial block: just able to flex knees with free movement of feet; III: Almost complete block: unable to flex knees, but with free movement of feet; IV: complete block: unable to move legs or feet); postoperative complications and total length of admission.
Data analysis
The collected data was analyzed using SPSS version 22.0 program. The results are expressed as mean ± SD or percentages and range. To analyze and compare the variables, non-parametric tests (Kruskal-Wallis, Mann-Whitney) were applied. Results were accepted as statistically significant when p < 0.05.
RESULTS
One hundred ninety-three medical records were reviewed. Six of them were excluded due to partial absence of data and one of them was excluded due to epidural catheter malfunction, requiring a switch to intravenous morphine for pain treatment.
Average surgery time was 161 ± 71 minutes (110-500 minutes, range). Anthropometric results and epidural technique results are available in Table I and Table II. Epidural infusion, rate and type of LA varied depending on the anesthesiologist's initial prescription and subsequent adjustments depending on the pain and side effects. LA used was levobupivacaine 0.125 % in 156 cases (85 % total); with fentanyl in 87 cases (46.8 % total) and without in 71 cases (38.2 % total). In the 28 (15 %) remaining cases, LA was bupivacaine, with fentanyl in 16 (8.6 %) and without in 12 (5.9 %) cases. In brief, in 55.4 % of the cases, LA + fentanyl was used, and LA without fentanyl in the remainder cases. No statistically significant differences in motor blockade between groups were seen (p > 0.05). Average infusion rate was 5.12 mL/h ± 1.1 mL/h.
TABLE I ANHTROPOMETRIC RESULTS OBTAINED FROM STUDIED SUBJECTS, DATA FROM ALL PATIENTS WHO UNDERWENT LAPAROSCOPIC RADICAL PROSTATECTOMY FOR PROSTATE CANCER BETWEEN 2010 AND 2015 WITH EPIDURAL ANALGESIA USED FOR POSTOPERATIVE PAIN TREATMENT
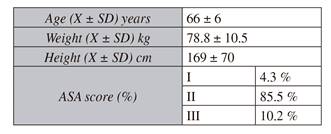
X: mean. SD: standard deviation. ASA: American Society of Anesthesiology.
TABLE II EPIDURAL TECHNIQUE RESULTS OBTAINED FROM STUDIED SUBJECTS, DATA FROM ALL PATIENTS WHO UNDERWENT LRP FOR PROSTATE CANCER BETWEEN 2010 AND 2015 WITH EPIDURAL ANALGESIA USED FOR POSTOPERATIVE PAIN TREATMENT
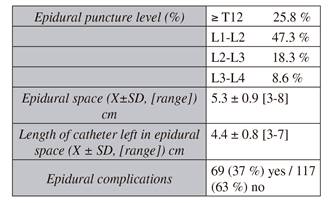
X: mean. SD: standard deviation.
Complications related to epidural technique appeared in 37 % of patients. Of all the technique-related complications there were 3 cases (1.5 %) of hematic puncture, and 1 (0.5 %) adverted dural puncture, in which technique was successfully repeated without further complications; 3 (1.5 %) accidental catheter disconnections after the first 24 h, where conventional analgesia was continued, as pain was well-controlled; and 1 (0.5 %) subdural block, with catheter removal and intravenous morphine used for pain relief (data relative to this patient was included up until that point). The subdural blockade and the dural puncture cases were strictly followed-up by the APU nurse, and no complications were observed.
As for neurological side effects, 56 patients (30.1 %) presented with motor block of one or both lower extremities after surgery, and 5 (2.7 %) with paresthesia. When talking specifically of the 56 patients with motor blockade, in 42 cases (75 %) it was a unilateral Bromage I degree block; and in 14 patients (25 %) it was a bilateral block (8 Bromage I and 6 Bromage II) (Table III).
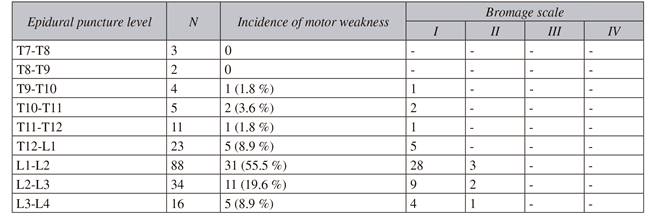
The highest frequency of motor weakness was observed during the first 6 to 12 hours after surgery. The degree of motor block in relation to the level of epidural puncture is shown in Table III. Motor weakness was greater in the epidural lumbar punctures than in thoracic level punctures, although results were not statistically significant. In the 42 cases of unilateral motor blockade (see previous results), the catheter was removed 0.5-1 cm, if possible, and the patient was placed on his side, with the blocked side on top. In all cases blockade was reversed. In the cases of bilateral block, the 8 Bromage grade I blocks were treated by decreasing the LA infusion rate; in the remaining 6 bilateral Bromage II patients, infusion was suspended until improvement, which was complete in all cases. In most cases catheter mobilization was performed at the PACU. In those cases of bilateral block, drug infusion was suspended until reversal of motor blockade was observed, at which point infusion was re-started at lower rates. These patients were controlled strictly by the APU nurse.
Postoperative pain
Patients were followed during the time epidural catheter was in place. Average VAS at rest (r) and upon movement (m) in PACU and on first, second and third day was r 0.7 ± 1.2, m 2.1 ± 1.7; r 0.8 ± 1.3, m 1.9 ± 0.9; r 0.61 ± 1.2, m 2.01 ± 1.7; and r 0.8 ± 1.1, m 1.78 ± 2; respectively (Figure 1). Overall, average VAS at rest was 1.2 ± 1.6; and upon movement, average VAS was 1.9 ± 1.8.
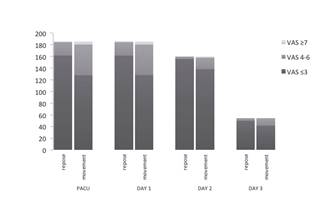
VAS: visual analog scale.
Fig. 1 Daily VAS in patients with epidural catheter for postoperative pain management of laparoscopic radical prostatectomy, evaluated upon repose and movement.
Epidural catheter remained in place for over 72h in only 5 % of the cases. 26 (14 %) patients required epidural analgesia for 24 h, 106 (57 %) for 48 h, and 44 (23.5 %) for 72 h. Of the 10 patients (5 %) were the catheter was maintained for over 96 h; in 8 cases it was due to surgical revision; and in 2 patients the infusion was stopped but catheter couldn't be removed due to abnormal clotting parameters due to excessive bleeding.
Postoperative care
Ten cases required hospital admission above 10 days, due to surgical complications. These were 4 cases of urinary leakage, 2 urinary tract infection cases, 1 surgical wound infection, 1 case of pulmonary embolism, 1 bladder dome section that coursed with anuria, and 1 paralytic ileus. There were 5 cases of postoperative bleeding treated conservatively. Length of hospital stay was 5.98 ± 2.92 (minimum 2 days and maximum 30 days).
Statistical analysis showed that motor weakness was not related to age, weight, type of LA used, addition of fentanyl, infusion rate, level of epidural puncture nor length of catheter within the epidural space (p > 0.05).
DISCUSSION
In LRP, the pain is defined as moderate 1. With the goal of increasing the welfare of postoperative patients undergoing this type of intervention, studies comparing open versus laparoscopic technique have been conducted, with inconclusive results. Results by Webster et al. 18 concluded that necessity of analgesics diminished if it the procedure is laparoscopic; whereas D'Alonzo et al. 19 did not find statistically significant differences between the two techniques in terms of opioid consumption.
Systematic reviews reveal a significant lack of evidence in the pain management protocol of patients undergoing LRP 5. Most studies evaluate pain under unimodal analgesic management 20, not multimodal management, as is the current trend. Moreover, while it is accepted that LPR decreases postoperative pain, studies are few. It is therefore necessary to determine the optimal analgesic technique for this type of surgery 2) (3) (4. Studies have shown that pain in this type of surgery can be controlled with opioids, but because of their side effects 2) (7, nowadays other analgesic techniques are advocated.
Since the opening of our center in 2010, control of postoperative pain in the LRP has been performed using lumbar epidural analgesia. The epidural technique allows for optimal pain control, improving patient comfort 8, reducing side effects of other analgesics 2) (7,and the number of complications such as postoperative infarction, bleeding, pulmonary comorbidities, respiratory depression, kidney failure, and deep vein thrombosis 21) (22) (23) (24) (25.
When evaluating our results (Figure 1), the average VAS at rest (1.2 ± 1.6) and on movement (1.9 ± 1.8) remained below 3 during follow-up in all patients. Although studies have been published that correlate younger age with a higher pain score 26, our VAS records were excellent, in spite of an average age of 66 years. However, the complications associated with this technique must be kept in mind: catheter infection, post-dural puncture headache, stroke, intracranial hematoma, cerebral thrombosis, meningitis, and neurological disorders 11), 27) (28. No major complications were recorded, but thirty-seven per cent of analyzed patients presented some type of minor complication.
As summarized in Table 3, 56 patients (30.1 %) had motor weakness, especially during the first 12 hours after surgery, which disappeared with standard maneuvers such as change in patient´s position and / or reduction or suspension of LA infusion. These results are similar to those published by Broekedema 16 et al. and Ahmed 27 et al. Broekedema 16 studied surgeries performed with either lumbar or thoracic epidural. A single motor blockade was detected in a patient with a lumbar epidural. Numbness could be detected in patients with either lumbar or low thoracic epidurals, with symptoms disappearing when infusion rate decreased. In the study by Ahmed et al. 27, 36.5 % of patients with local anesthetic epidural infusion presented motor weakness. The most likely cause of this initial motor blockade is attributed to the persistence of effect of LA administered during the surgery 12. Regarding the incidence of motor block according to puncture level, we observed that this is higher at lumbar (74.2 %) versus thoracic (25.8 %) level (p > 0.05); being these results similar to those described in other studies 11) (27. This is thought to be due to anatomical reasons.
In addition to motor block, 5 cases of paresthesias, 3 hematic punctures, 3 accidental catheter disconnections (with consequent sterility loss) and 1 dural puncture were recorded. In 2 of the 5 cases of postoperative bleeding, the catheter was not removed until the 5th day due to coagulation disorders, and in the case of bladder dome section, it wasn't removed until the 8th day. Although risk of infection due to prolonged catheter placement is described as low 28, it nonetheless increases when catheter isn't timely removed. Vascular punctures, unnoticed in 9 % of the cases 29, can lead to disastrous consequences (hemodynamic disturbances, heart failure). Other complications include urinary retention 28 or direct spinal cord injuries. For this reason, several studies advocate for other analgesic techniques 30) (31.
Even if epidural technique covers pain in LRP excellently, the current trend is toward drain-less, less invasive surgery. This tendency raises the question of whether such analgesic technique is really necessary for lower abdominal surgeries, taking into account not only possible complications but also increased costs associated with epidural follow-up 32. Moreover, despite the advantages of the epidural technique, there is a lack of evidence to support its superiority over intravenous analgesia. While there are studies that advocate the benefits of epidural analgesia technique 33, others find no superiority in comparison to systemic analgesia 20.
In addition to this, we must remember that the current trend is the implementation of Fast-track protocols, in order to obtain patient's early discharge and a return to normal life as quickly possible 1) (8) (9 .
Fast-track protocols are new multimodal approaches that deviate from standard treatments that include an increased fluid administration, use of nasogastric tubes and post-operative drains, prolonged postoperative oral intake restriction and immobilization; in order to favor early discharge and decrease hospital length-of-stay 34. The fact that LRP is not a bowel procedure favors the implementation of Fast-track therapy. As well as the use of minimally invasive techniques associated to a decrease in inflammatory response and immunological dysfunctions, opioid-free anesthetic and / or analgesic techniques are advocated, minimizing postoperative complications and facilitating recovery 8) (9) (35 . Early-recovery-after surgery (ERAS) protocols have been included in various surgical paths 36) (37) (38, with scarce bibliography in urologic surgeries 39.
After reviewing the published literature, we decided to carry out a study comparing the epidural technique with another analgesic technique. In this context, we decided to evaluate the data of the epidural technique of the previous 5 years.
Epidural technique fulfills the requirements for analgesia in Fast-track surgery, providing optimal pain control with minimal opioid administration, as seen in our study and in the literature. However, it has its drawbacks, as it may hinder early mobilization when paresthesia, motor blockade or other complications appear; and hospital costs related to monitoring of these complications increase. Neural block, not only epidural technique but any local technique that blocks nerve impulses, inhibits the endocrine and sympathetic response to surgery, more effectively in lower than in upper abdominal surgery 40. Thus, epidural benefits can be obtained with other neural blockade analgesic techniques, avoiding possible complications.
Our average length-of-stay is 5.98 ± 2.92 days. Magheli et al. found that with the implementation of the Fast-track protocol in the LRP, hospital stay was reduced from 7 days to 3.7 days, and complication rate decreased 1. However, recent studies demonstrate that epidural analgesia increases length-of-stay 41) (42. We cannot assure that the average hospital stay could have been lower if another analgesic technique had been performed, but after analyzing the complications obtained would be an important factor to take into account. To clarify these data, comparative studies between the epidural technique and new anesthetic techniques would be necessary, which is what we are currently undertaking. For example, several studies supporting TAP block as an analgesic technique in colorectal surgery have been published 30) (31. McDonell et al. 43 evaluated the TAP blockade in colorectal surgery and obtained very good pain control. In a meta-analysis, which evaluated the TAP blockade as analgesic technique in laparoscopic surgery, it concluded that TAP technique is an effective analgesic technique in patients undergoing laparoscopic Fast-track surgery, providing analgesic quality without associated complications 44. However, specific literature regarding TAP block in LRP is scarce.
Our study has some limitations. Being an observational retrospective study, anesthesia management of patients did not follow strict protocols and this produces an important bias. Furthermore, data was collected retrospectively, with some data missing, compromising data analysis and reducing power of statistical conclusions. Motor blockade was greater in those patients with lumbar catheters than those with thoracic catheters, as has been previously described 12) (25) (27, but we can only speak of tendencies, as there was no technique randomization, and results may be subject to bias. The same is applicable when considering the use of fentanyl.
Ideally, the epidural technique should be compared to the new emerging analgesic techniques, as retrospective studies hinder the association of causality between variables. We are currently carrying out a comparative, prospective study, to reduce these bias.
CONCLUSION
To conclude, the epidural technique offers an excellent analgesic quality, but complications and/or side effects associated to the use of LAs disagree with the terms of Fast-track surgery, with risk of increased length-of-stay. Other analgesic techniques may offer the same pain management without the complications of the epidural technique.

