










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAnales del Sistema Sanitario de Navarra
Print version ISSN 1137-6627
Anales Sis San Navarra vol.36 n.1 Pamplona Jan./Apr. 2013
https://dx.doi.org/10.4321/S1137-66272013000100022
Infiltrating gastric adenocarcinoma with disseminated osteoblastic metastases
Adenocarcinoma gástrico infiltrante con metástasis osteoblásticas diseminadas
V.M. Santos1,2, T.A. Vieira2, C.S. Marinho2, T.P. Loures2, B.B.V. Brandao2, R.N. Botan3
1. Catholic University Medical Course. Brasília-DF. Brazil.
2. Internal Medicine Department of Armed Forces Hospital. Brasília-DF. Brazil.
3. Oncology Division of Armed Forces Hospital. Brasília-DF. Brazil.
Dirección para correspondencia
ABSTRACT
We report the case of a man with a diagnosis of invasive gastric adenocarcinoma associated with scattered osteoblastic metastases. This 65-year-old patient was admitted with nausea, vomiting and abdominal pain, in addition to loss of weight (13 Kg in 3 months). Upper digestive endoscopy revealed extensive infiltrating changes in the body of the stomach, and histopathologic data confirmed the diagnosis of a Borrmann IV gastric adenocarcinoma. Complementary exams were indicative of a gastric cancer with bone metastases, characterized by disseminated osteoblastic images of the scintigraphy of the skeleton. Palliative chemotherapy was the treatment of first choice. High serum levels of CA 19-9, CEA and alkaline phosphatase can constitute useful indicative tools of this challenging condition. Images from a scintigraphy study of the skeleton can characterize the type and extension of bone metastases. The aim of this case study is to report a case of a very uncommon condition, considering that disseminated osteoblastic metastases rarely develop in this kind of tumor.
Key words. Adenocarcinoma. Bone metastasis. Gastric tumor.
RESUMEN
Presentamos un caso de adenocarcinoma gástrico infiltrante asociado con metástasis osteoblásticas diseminadas. Un paciente de 65 años ingresó con náuseas, vómitos y dolor abdominal asociados con pérdida de peso (13 Kg en 3 meses). La endoscopia digestiva objetivó extensas alteraciones infiltrativas del cuerpo gástrico y los datos histopatológicos confirmaron el diagnóstico de adenocarcinoma gástrico Borrmann IV. Exámenes complementarios fueran indicativos de cáncer gástrico con metástasis óseas, caracterizadas por imágenes osteoblásticas diseminadas de la cintilografía del esqueleto. Se le administró quimioterapia paliativa como primera opción. Se elevó CA 19-9, CEA y apareció fosfatasis alcalina en el suero un indicador útil del diagnóstico. La extensión y el tipo de metástasis óseas pueden ser imágenes de cintilografías del esqueleto. Este caso tiene como objetivo describir la presencia de metástasis osteoblásticas diseminadas que raramente son producidas por este tipo de tumor.
Palabras clave: Adenocarcinoma. Metástasis óseas. Tumor gástrico.
Introduction
Since 1995, mortality by cancer has been the leading cause of death among males in Navarre; while the incidence and mortality rates of gastric cancer have decreased1. In Spain, estimates and projections about the above mentioned rates for 2012 are indicative of a downward tendency2. Clinically unsuspected gastric adenocarcinoma has been reported in young and old individuals, with diagnosis established exclusively through autopsy studies3. Paraneoplastic phenomena and bone marrow implants can precede the diagnosis, which may be confirmed in advanced stage3-5. Worth of note, the «oldest old» population is growing both in industrialized and developing countries; therefore, one should consider the possibility of further increase in malignancy rates1,2. It is estimated that near 60% of people with cancer will have bone metastases, which frequently are not demonstrated during their life; fact that poses difficulties to establish the real incidence4. Bone metastasis is most frequently due to cancers from prostate, breast, kidney, lung and thyroid4. Autopsy studies describe skeletal metastases in only 5% of patients with gastrointestinal cancers, and osteoblastic implants of primary gastric cancer are considered a very uncommon finding4. The objective of this case study is to report an advanced gastric cancer associated with disseminated osteoblastic metastases, a probably under recognized and under reported condition.
Case report
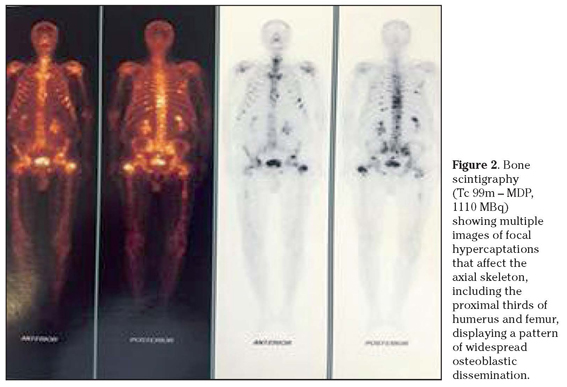
A 65-year-old man with arterial hypertension and diabetes mellitus was admitted because of inappetence and weight loss (13 Kg in 3 months), associated with nausea, vomiting and epigastric pain for 15 days. He denied alcoholism and tobacco smoking. Physical examination showed BMI of 24.2 kg/m2 and pale mucosa. No visceromegaly nor lymph node enlargement were observed. Prostate examination revealed a fibroelastic organ with 30g of estimated weight and absence of nodules. Upper digestive endoscopy showed extensive changes on the gastric body, compatible with diffuse infiltration by a highly advanced gastric adenocarcinoma - plastic linitis (Fig. 1A). Histopathology study of biopsy sample revealed a diffuse pattern adenocarcinoma (Fig. 1B). Laboratory tests and imaging studies were performed. Hemoglobin: 13.1g/dl, hematocrite: 39.9%, MCV: 79fl, MCH: 33%, leukocytes: 8,581/mm3, platelets: 423,000/mm3, glucose: 232 mg/dl, calcium: 9.1 mg/dl, sodium: 140 mmol/dl, potassium: 3.8 mmol/l, urea: 13.8 mg/dl, creatinine: 0.7 mg/dl, ALT: 13 U/L, AST: 9.6 U/L, alkaline phosfatase: 138 U/L, albumin: 3.33 g/dl, total PSA: 0.787 ng/ml, free PSA: 0.104 ng/dl, CA 19-9: 385.6 U/ml, and CEA: 14.1 ng/ml. CT images with contrast of abdomen revealed multiple osteoblastic implants in vertebral bodies (Fig. 1C) and in pelvic bones. Scintigraphy showed multiple focal hypercaptations on the axial skeleton, and proximal thirds of right humerus and left femur, with features of osteoblastic metastases (Fig. 2). Further investigations about differential diagnosis included routine tumor markers, and specific biochemical determinations related to neuroendocrine tumors, in addition to imaging studies by PET/ CT of the thorax and the head, which revealed unremarkable findings. With diagnosis of unresectable gastric adenocarcinoma, the patient underwent a palliative docetaxel + 5-fluorouracil + cisplatin (DCF) combination chemotherapy and, after hospital discharge, he was referred to regular outpatient surveillance at the Oncology Division.

Discussion
The incidence of gastric cancer is lowering in industrialized countries, but remains elevated in developing regions, with a higher prevalence amongst males5,6. Extension of disease to the adjacent organs constitutes the most common way of this tumor dissemination. Lymphatic metastases first occur to regional and latter to the distant lymph nodes; peritoneal carcinomatosis is the most common site of distant metastasis, followed by the liver, lungs and bones5. Bone metastases are found between 1% and 20% of cancers of the stomach5,7-9, and are mainly osteolytic, while osteoblastic implants are considered rare5-10. Notwithstanding, an exceeding rare case of osteoblastic metastases was described in an early gastric cancer - confined to the mucosa and submucosa, which evolved to death 18 months after surgery due to generalized disease10. Osteoblastic metastases are characteristic of prostate cancer, but may occur in other malignancies like carcinoide, gastrinoma, small cell lung cancer, medulloblastoma, astrocytoma, glioblastoma, thymoma, cancers of breast, kidney, thyroid, colon, pancreas, nasopharynx, and urinary bladder, and Hodgkin's lymphoma. Bone metastases may be demonstrated by images of CT, magnetic nuclear resonance, and scintigraphy6,7. The diagnosis of fourth Borrmann type8, also designated scirrhous gastric carcinoma and linitis plastica was established in this case study. During the staging of the tumor, scattered osteoblastic metastases were detected by CT imaging studies of abdomen, and were further confirmed by the findings from the scintigraphy of skeleton6,7. Neither gastrectomy by laparotomy, nor by laparoscopy, were considered good options for treatment of this patient with base on the risk/benefit balance11. The choice of DCF as the palliative chemotherapy schedule in the present case was based on the remarkable survival benefit described for patients with advanced adenocarcinoma of the stomach12. Bone metastasis associated with gastric cancer is considered a relatively uncommon phenomenon4,5, and has been related to poorer prognosis6,9, in special if implants occur in multiple areas6,8,9. Asymptomatic bone implants occur in up to 20% of the patients with gastric cancer, but main symptoms are pain, fractures, and paraplegia9. Laboratory tests indicative of gastric cancer with bone metastasis include high serum levels of alkaline phosfatase, CA 19-9 and CEA6-9. The data (normal range in parenthesis) in our patient were 138 (40-130) U/L, 385.6 (< 34) U/ml, and 14 (< 5) ng/ml), respectively. Interestingly, a significant relationship was found between the occurrence of lymphatic dissemination of gastric cancer and concomitant bone implants, in addition to a short survival6,13. Notably, osteoblastic flares have been reported in patients with advanced gastric cancer submitted to antitumor therapy7, however, we detected the implants before the cytotoxic regimen. Major concern was the finding of osteoblastic implants in an old male patient, which raised the initial hypothesis of a primary prostate cancer4,6. Nevertheless, he was accurately evaluated by specialists in Urology, and his serum levels of total and free PSA were found within the respective normal ranges. Therefore, the hypothesis of a concomitant prostate cancer was ruled out. Furthermore, no indicative feature of other coexistent malignancy was detected.
The purpose of this report is to enhance the awareness of non specialist physicians about the possible occurrence of osteoblastic metastasis in advanced gastric cancer, emphasizing the levels of alkaline phosfatase, CA 19-9 and CEA as useful tools for clinical suspicion, and the scintigraphy imaging of skeleton for accurate evaluation of the involved bones.
References
1. Ardanaz E, Moreno-Iribas C, Pérez De Rada ME, Ezponda C, Flaristán Y, Navaridas N, et al. Incidencia y mortalidad por cáncer en Navarra, 1998-2002. Evolución en los últimos 30 años. An Sist Sanit Navar 2007; 30: 245-270. [ Links ]
2. Sánchez MJ, Payer T, De Angelis R, Larrañaga N, Capocaccia R, Martinez C for the CIBERESP Working Group. Cancer incidence and mortality in Spain: estimates and projections for the period 1981-2012. Ann Oncol 2010; 21: iii30-36. [ Links ]
3. Santos VM, Castro ECC, Araújo AC, Reis MA, Teixeira VPA. Budd-Chiari syndrome and unsuspected gastric adenocarcinoma. Medicina (Ribeirão Preto) 2005; 38: 156-160. [ Links ]
4. Maccauro G, Spinelli MS, Mauro S, Perisano C, Graci C, Rosa MA. Physiopathology of spine metastasis. Intern J Surg Oncol 2011; 107969. Epub 2011 Aug 10. [ Links ]
5. Escuissato DL, Ledesma JA, Urban LABD, Liu CB, Reis Filho JS, Oliveira Filho ag et al. Metástase de câncer gástrico simulando neoplasia primária de pulmão - relato de caso e revisão da literatura. Radiol Bras 2002; 35: 121-124. [ Links ]
6. Ahn JB, Ha TK, Kwon SJ. Bone metastasis in gastric cancer patients. J Gastric Cancer 2011; 11: 38-45. [ Links ]
7. Amoroso V, Pittiani F, Grisanti S, Valcamonico F, Simoncini E, Ferrari VD, et al. Osteoblastic flare in a patient with advanced gastric cancer after treatment with pemetrexed and oxaliplatin: implications for response assessment with RECIST criteria. BMC Cancer 2007; 7: 94. [ Links ]
8. Cchung YS, Choi TY, Ha CY, Kim HM, Llee KJ, Ppark CH, et al. An unusual case of osteoblastic metastasis from gastric carcinoma. Yonsei Med J 2002; 43: 377-380. [ Links ]
9. Marti J, Sainz M. Unusual late metastasis from gastric carcinoma. Saudi J Gatroenterol 2011; 17: 423-424. [ Links ]
10. Anagnostopoulos G, Sakorafas GH, Kostopoulos P, Margantinis G, Tsiakos S, Pavlakis G. Early (mucosal) gastric cancer with synchronous osteosclerotic bone metastases: a case report. Eur J Cancer Care (Engl) 2010; 19: 554-557. [ Links ]
11. Ibáñez FJ, Azagra JS, Goergen M, Bordas JM, Almendral ML, Erro JM. Cirugía laparoscópica del cáncer gástrico. An Sist Sanit Navar 2005; 28: 21-31. [ Links ]
12. Ben Aharon O, Purim O, Kundel Y, Brenner R, Gordon N, Sulkes A, et al. The combination of docetaxel, cisplatin, and 5-fluorouracil in advanced gastric cancer: a single-institution experience. Anticancer Drugs. 2012 Jan 10. (Epub ahead of print) [ Links ]
13. Kong JH, Lee J, Yi CA, Park SH, Park JO, Park YS, et al. Lung metastases in metastatic gastric cancer: pattern of lung metastases and clinical outcome. Gastric Cancer 2011; Oct 29. (Epub ahead of print) [ Links ]
![]() Dirección para correspondencia:
Dirección para correspondencia:
Vitorino Modesto dos Santos
Armed Forces Hospital
Estrada do Contorno do Bosque, s/n
Cruzeiro Novo
70658-900, Brasilia. Brazil
E-mail. vitorinomodestos@gmail.com
Recepción: 27 de junio de 2012
Aceptación provisional: 18 de octubre de 2012
Aceptación definitiva: 30 de octubre de 2012

