










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
According to the last estimations provided by the International Agency for Research on Cancer (IARC), prostate cancer was the second most common cancer diagnosed in men worldwide in 2012, accounting for 15% of the cancer cases. Almost 70% of them occurred in developed regions, where prostate specific antigen (PSA) testing and subsequent biopsy are widespread1. The PSA testing has a big effect on incidence rates and therefore the rates can vary among different countries according to the level of PSA implementation. Prostate cancer incidence has increased in recent decades in Europe2. As far as mortality is concerned, 307,000 deaths were estimated worldwide in 2012, placing prostate cancer as the fifth leading cause of death from cancer in men (6.6% of the total men deaths). The mortality rates are less variable among different regions worldwide3.
As in other European countries, prostate cancer is the most frequent cancer in Spain among men. In 2015, according to the last estimations provided by Galcerán and col 4 33,370 cases were diagnosed in Spain. Prostate cancer mortality is placed as a third cause of death by cancer in men after lung and large bowel cancer 4, 5.
The objective of this study is to provide an in-depth description of trends of prostate cancer in Navarra. To do so, the most up-to-date population-based incidence and mortality data were used. The study is focused on the observed overall and age-specific incidence and mortality trends. Additionally, projections of the incidence and mortality rates are provided up to 2016 as an updated indicator of the burden of this cancer in Navarra.
METHODS
Data on the incidence of invasive prostate cancer were obtained from the population-based Cancer Registry of Navarra, a region in northern Spain with a population of approximately 640,000 inhabitants in 2010 in which almost 50% were men. We used the most up-to-date prostate cancer incidence data available in the cancer registry, covering the period 1975-2010. The Navarra Cancer Registry uses multiple sources of information on cancer, including pathology laboratories, hospitals and death certificates. Mortality data from 1975 to 2013 were provided by the Spanish Statistical Office6. Population data by 5-year age groups and gender were obtained from the Statistical Institute of Navarra7.
A brief descriptive analysis is provided computing the total number of cases, the average number of cases per year with the standard deviation and the maximum and minimum number for the first and last ten years period of study for the total population and for 45-74 and older than 74 (75+) year age-groups (results for age-group below 45 years were not provided in the descriptive analysis due to the small number of cases).
Annual age-standardized incidence and mortality rates were calculated by the direct method using the new revised European Standard Population 20138. Trends in incidence and mortality rates were analyzed and change-points and annual percentage changes (APC) were estimated by joinpoint regression analysis using Joinpoint Trend Analysis Software 4.2.0.2 9, 10. The estimates and p-values for the annual percentage changes (APC) were estimated as 100*(exp(β)-1), where β is the slope of the following log-linear regression model ln(y)= β0 + β1*t, where t is the variable time. The p-value of the APC comes from a two-sided test for regression slope which is based on a t distribution9. These analyses were carried out for the whole population and for 45-74 year and 75+ year age-groups.
One-dimensional P-spline models were used to estimate projections of the prostate cancer incidence and mortality rates up to 2016. In order to obtain the best estimations, the models were fitted in different periods: 1989-2010, 1990-2010, 1991-2010, and so on. Then, a validation process was carried out, in order to assess the predictive performances of models. In this process, the mean absolute relative bias (MARB) was computed for each fitting. This measure indicates which time period is the best to provide the best predictions. Values close to cero indicate good performance of the model11. The MARB indicated that 1999-2010 period was the best to predict incidence rates and 1996-2013 period was the best to predict mortality rates. The mean MARB values for incidence and mortality predictions where 0.0484 and 0.0759.
RESULTS
A total of 7,707 incident cases of invasive prostate cancer were recorded in the twenty-five year period and 1,629 prostate cancer deaths occurred in the twenty-eight year period analysed. Incidence and mortality in the first and the last ten years of the study period are shown in Table 1. The annual number of incident cases markedly increased between these two periods from 83 to 377. By age-groups the absolute number of incident cases rose from 42 to 248 in men 45-74 years old and from 41 to 129 in men aged 75+. Similarly, an increase in the absolute number of prostate cancer deaths was observed between the two periods.
Table 1 Prostate cancer incidence and mortality in the first and last ten years of the study period for the total population and by age-groups in Navarra
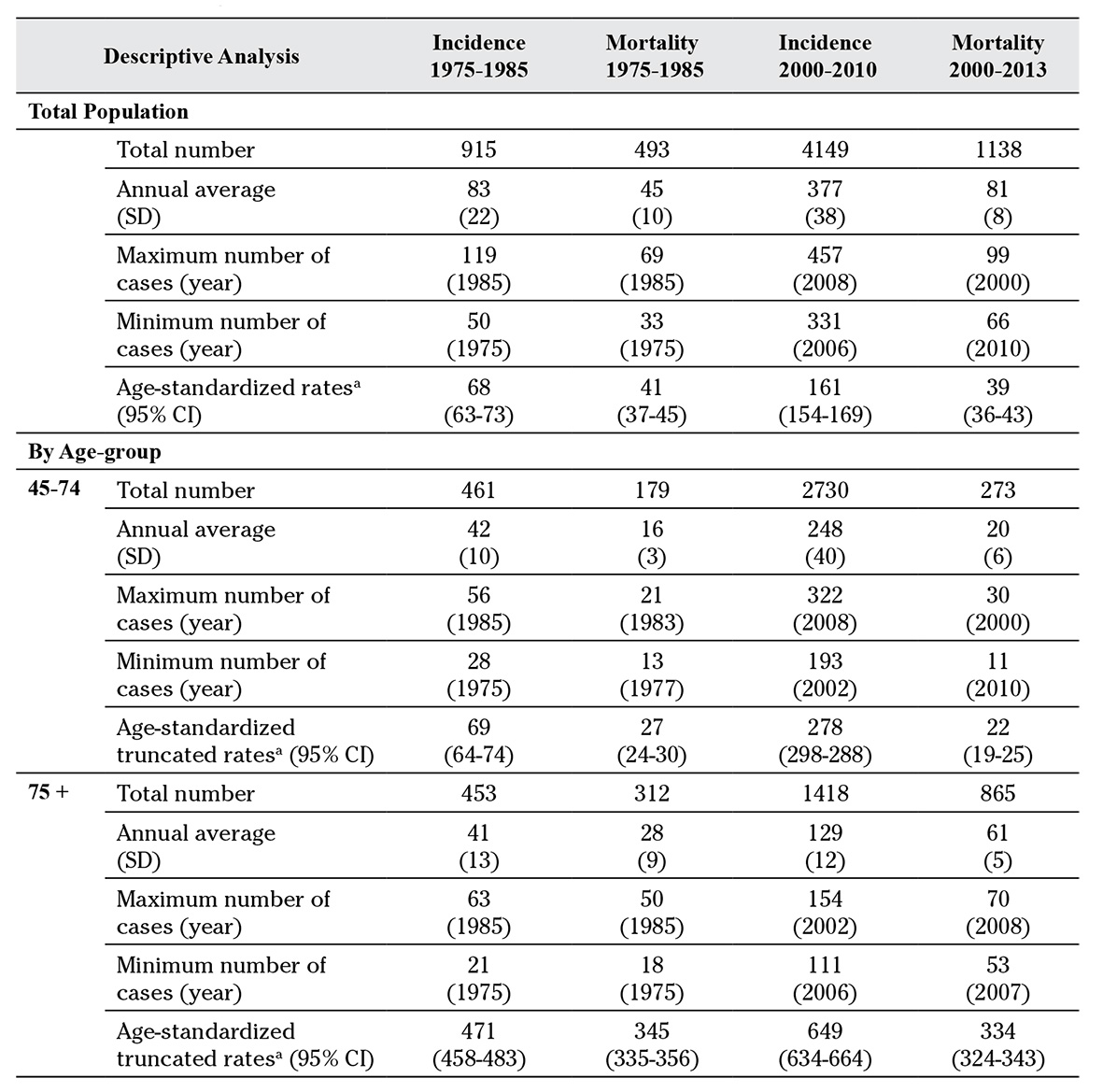
SD: standard deviation; a: annual mean; 95% CI: confidence interval; 75+: 75 years or older
Trends in age-standardized incidence and mortality rates for the whole population are shown in Figure 1. Prostate cancer incidence rates increased by 4.1% annually between 1975 and 2002 (p<0.001) followed by a stabilization of rates until 2010 (APC +0.7%, p=0.726); therefore, a change point in incidence was estimated in 2002. On the other hand, the mortality rates showed an increase of 2.2% (p<0.001) per year up to 1995, while a decreasing trend (APC -3.4%, p<0.001) was observed up to 2013.
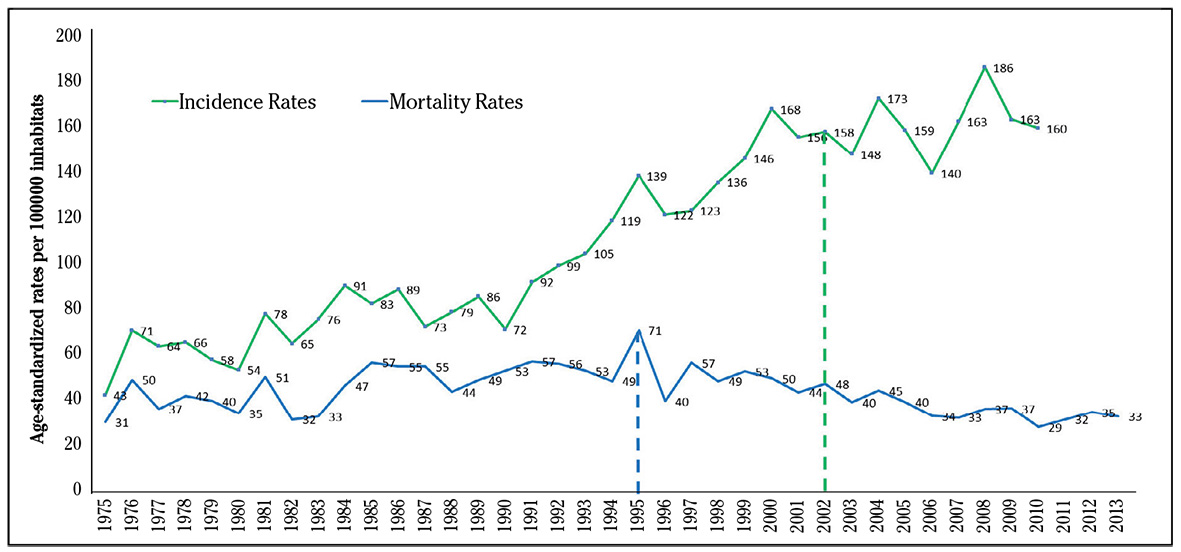
Figure 1 Trends and change points in age-standardized incidence and mortality rates of prostate cancer in Navarra.
Age-specific incidence rate trends for 45-74 and 75+ age-groups are shown in Figure 2. An increase in incidence was observed in the 45-74 age-group over the studied period. More precisely, incidence rates increased by 4.5% annually from 1975 to 1990 (p<0.001), then by 9,6% per year up to 2000 (p<0.001), followed by a less pronounced increase up to 2010 (APC +2.4%, p=0.023). In the 75+ age-group, an increase of rates was observed between 1975 and 1999 (APC +3.3%, p<0.001), followed by a significant decrease (APC -4.0%, p<0.01). Mortality trends were quite similar in the two age-groups. The mortality rates for the 45-74 age-group increased up to 1994 (2.9% per year, p<0.01), afterwards a significant decline was observed up to 2013 (APC -4.7%, p<0.001). In the 75+ age-group mortality rates increased up to 1995 (2.5% per year, p<0.001) and then declined up to 2013 (APC -3.6% per year, p<0.001).
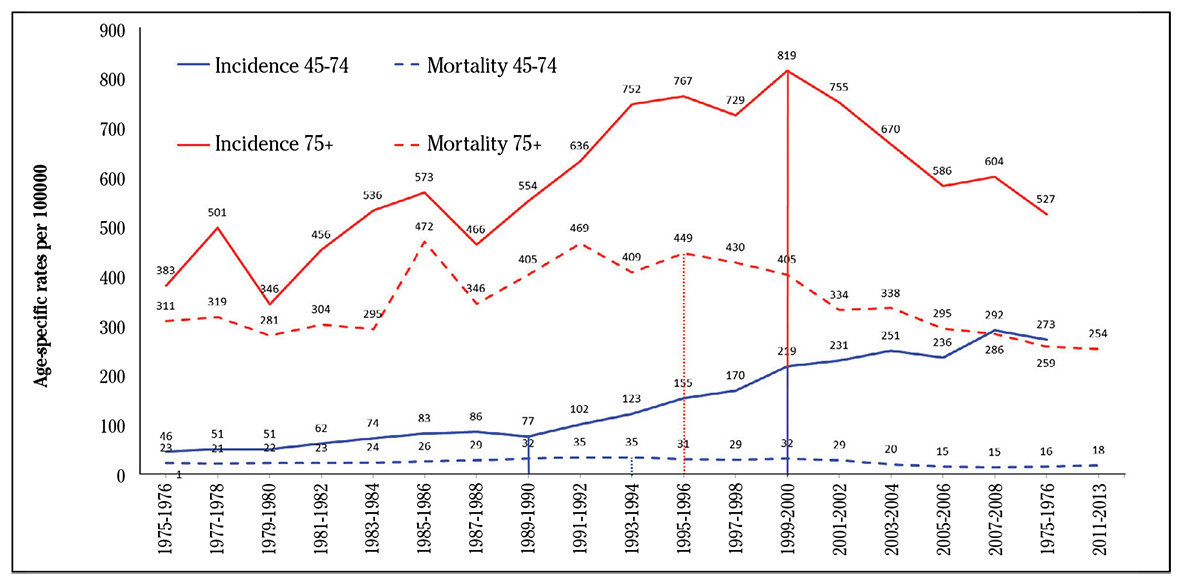
Figure 2 Trends and change points in age-standardized incidence and mortality rates of prostate cancer by age-groups (45-74 and 75 or older) in Navarra.
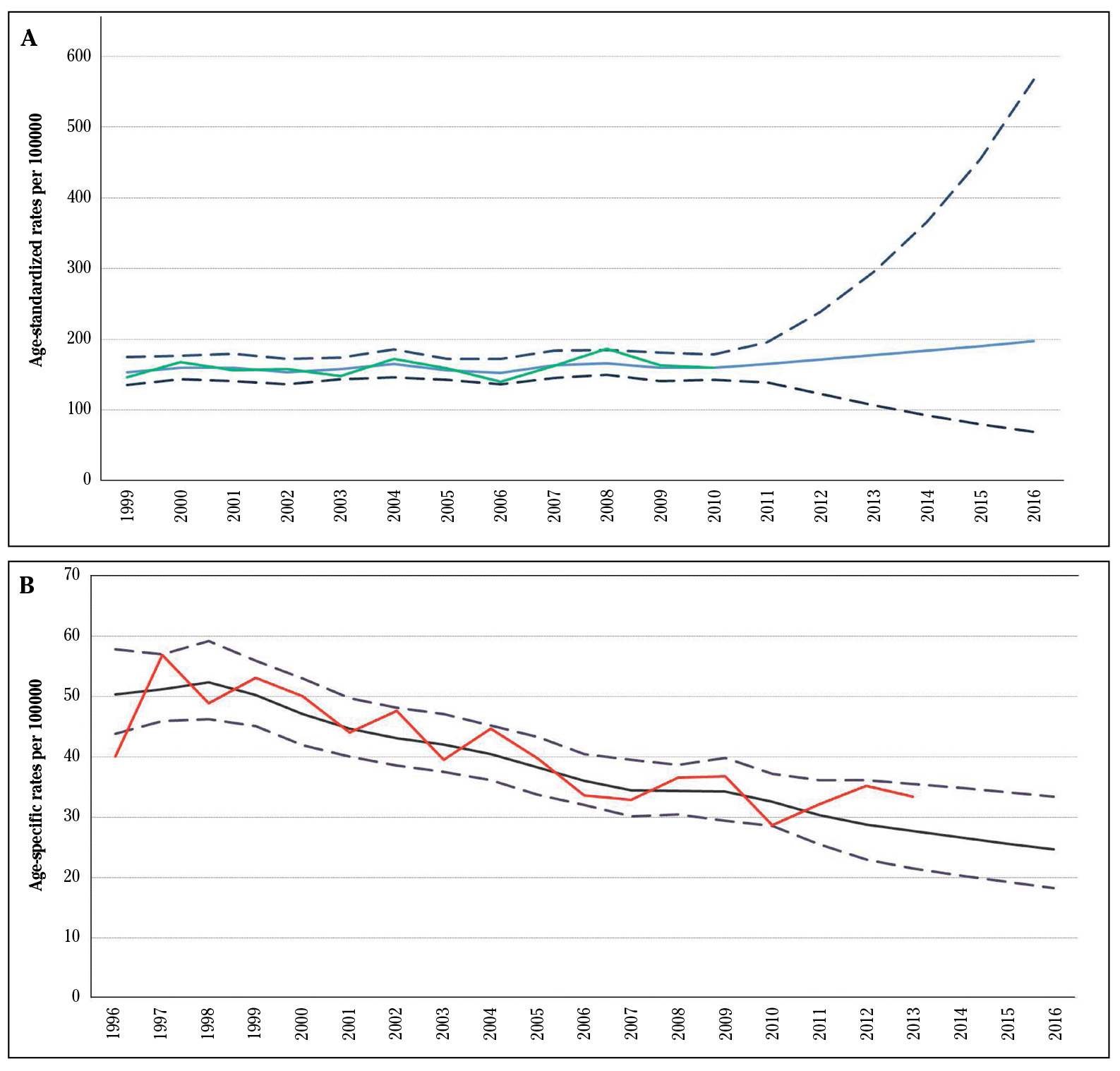
Estimated projections for prostate cancer incidence and mortality up to 2016 based on one-dimensional P-spline models were represented in Figure 3. It is estimated a slight increase of incidence rates while the reduction of mortality would have continued up to 2016.
DISCUSSION
In this study, prostate cancer incidence and mortality trends were analyzed throughout a large period in Navarra. In recent years, even though overall incidence rates stabilized from 2002 to 2010, trends were different between the two age groups analyzed: rates increased in 45-74 years old age-group and decreased in the older age-group. A decline in mortality was observed in both age groups since about 1995.
Overall changes in incidence and mortality observed in Navarra are similar to those reported in Spain and other European countries 5, 12, 13, 14. In Spain, incidence rates increased by 1.3% per annum from 1975 to 1990, and even more sharply thereafter (7.3% per annum) up to 200413. The sharp rise in incidence after the early 1990s observed also in countries such as the United States and other European countries coincided with the introduction of PSA testing 15, 16, 17,18. Some authors have suggested that the increase of incidence may also be attributed to the more frequent use of transurethral resection of the prostate and invasive diagnostic procedures such as random biopsies16.
An outstanding finding in Navarra incidence trends, not reported previously in Spain, is the decrease of the cancer incidence observed in men 75+ years old. This decline in the incidence has been observed in men older than 80 years in the United Kingdom19, as well as in the United States20. In this last country, a recent study showed a decline in the incidence not only in the older but also in younger age groups since 2011, and according to the authors this decrease could be related to the decreased PSA screening after the publication of the results from two large clinical trials: the prostate, lung, colorectal and ovarian (PLCO) cancer screening trial and the European randomized study of screening for prostate cancer (ERSPC)21.
Several authors have discussed about different changes in care of prostate cancer patients and their contribution in the decline of prostate cancer mortality: increase in the use of higher-definition computed tomography and ultrasonography for a better diagnosis and staging, more refined surgical approaches, introduction of antiandrogen therapies, chemotherapy and new modes of radiation treatment, and the use of PSA for diagnosis and monitoring to detect locally recurrent or metastatic disease before it becomes symptomatic 22, 23.
Based on the observed period, incidence rates are projected up to 2016. However, since the prostate cancer incidence is very sensitive to PSA screening, changes in screening practices could affect markedly these predictions. Currently, the Sociedad Española de Medicina Familiar y Comunitaria (semFYC), the Canadian Task Force on Preventive Health, the UK National Screening Committee and the US Preventive Services Task Force, among other scientific institutions, do not recommend PSA-based systematic screening for prostate cancer in asymptomatic population. These recommendations are supported by studies measuring pros and cons of early detection and subsequent treatment of localized prostate cancer. Additionally, there are no evidences indicating that prostate cancer patients diagnosed by screening have better outcomes than those diagnosed from clinical symptoms. Furthermore, it should be taken into account the important risks associated with PSA screening, including the risks of overdiagnosis and overtreatment24.
In conclusion, overall prostate cancer incidence rates seem to have stabilized in 2002-2010 in Navarra, however, trends were different by age groups: increased in men 45-74 years old whereas decreased in the 75+ year age-group. A decline in mortality rates was observed in both age groups since about 1995. Changes in the use of PSA test for screening in oncoming years could affect future prostate cancer trends.

