










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkPediatría Atención Primaria
versão impressa ISSN 1139-7632
Rev Pediatr Aten Primaria vol.16 no.64 Madrid Out./Dez. 2014
https://dx.doi.org/10.4321/S1139-76322014000500004
Influence of sex and school type on overweight and obesity rates
Influencia del sexo y el tipo de escuela sobre los índices de sobrepeso y obesidad
D. Arriscado Alsinaa, J. J. Muros Molinab, M. Zabala Díazc, J. M. Dalmau Torresa
aDepartamento de Ciencias de la Educación. Universidad de La Rioja. Logroño, Spain.
bDepartamento de Nutrición y Bromatología. Universidad de Granada. Granada, Spain.
cDepartamento de Educación Física y Deportiva, Universidad de Granada. Granada, Spain.
ABSTRACT
Introduction: child overweight and obesity have become, in recent decades, an epidemic that affects developed countries in particular. Many increasingly negative health impacts are related to childhood obesity. The aim of this study was to determine the prevalence of overweight and obese people in a city of northern Spain, and to identify the factors that influence this prevalence and its relationship with blood pressure.
Material and methods: the study was conducted on a representative sample of 329 sixth-grade students (11-12 years) from the city of Logroño. Socio-demographic data, blood pressure, maturational development, body mass index, waist and hip circumferences, and triceps and subscapular skinfolds were obtained.
Results: in all anthropometric measurements significant differences between people of average weight and overweight/obese people were found. The prevalence of overweight and obese people, according to international benchmarks, was 23.7% and 3.3%, respectively. This prevalence was higher in boys and students in public schools. Significant relationships between anthropometric variables and both systolic and diastolic blood pressure were found.
Conclusions: the rates of overweight and obese people were similar to the rest of the country, with the highest rates found in male students and in those educated in public schools.
Key words: Sex; Primary schools; Blood pressure; Obesity; Overweight.
RESUMEN
Introducción: el sobrepeso y la obesidad infantiles han pasado a ser, en las últimas décadas, una epidemia que afecta especialmente a los países desarrollados. Cada vez son más las repercusiones negativas sobre la salud que tienen relación con la obesidad infantil. El objetivo de este estudio fue determinar las prevalencias de sobrepeso y obesidad de una ciudad del norte de España, así como identificar los factores que influyen en la misma y la relación existente con la tensión arterial.
Material y métodos: el estudio se llevó a cabo sobre una muestra representativa compuesta por 329 escolares de sexto curso de primaria (11-12 años) de la ciudad de Logroño (La Rioja, España). Se obtuvieron datos sociodemográficos, tensión arterial, desarrollo madurativo, índice de masa corporal, perímetros de cadera y cintura, y pliegues de tríceps y subescapular.
Resultados: en todas las medidas antropométricas se encontraron diferencias significativas entre los normopesos y los sobrepesos/obesos. Las prevalencias de sobrepeso y obesidad, según referencias internacionales, fueron del 23,7 y el 3,3%, respectivamente. Estas prevalencias fueron mayores en niños y en alumnos de las escuelas públicas. Se encontraron relaciones significativas entre las variables antropométricas y la tensión arterial, tanto sistólica como diastólica.
Conclusiones: los índices de sobrepeso y obesidad fueron similares a los del conjunto de la nación, siendo los casos con mayor prevalencia los de alumnos de sexo masculino y los escolarizados en centros públicos.
Palabras clave: Sexo; Escuelas primarias; Presión arterial; Obesidad; Sobrepeso.
Introduction
Obesity is considered an epidemic and one of the greatest health problems of the twenty-first century,1 the consequences of which could lead to a decrease in life expectancy.2 In this regard, the significant increases in the prevalence rates of childhood overweight and obesity documented in recent decades in most developed and developing countries3 are particularly relevant. Spain is one of the countries with the highest prevalence rates of childhood overweight and obesity in Europe4, and the prevalence of childhood obesity in the autonomous community of La Rioja in particular is slightly above the national average at 9.7%.5 These data are alarming, as a relationship between excess weight in the early years of life and the presence of excess weight in adolescence6 and adulthood7 has been clearly established.
There is a growing number of studies that associate childhood overweight with dyslipidaemia,8 insulin resistance and type 2 diabetes,9 or psychosocial morbidity.10 Overweight also promotes the development of metabolic syndrome,11 defined as a cluster of risk factors for cardiovascular disease, including high blood pressure.12 Different studies point at sedentary behaviours,13 lack of physical activity, especially vigorous activity,15 and contemporary dietary habits16 as the main causes of excess fat accumulation. Then again, these habits are themselves influenced by multiple factors. Among the most important are sociodemographic factors17 such as sex, socioeconomic level, or the type of school the child attends. But there is also evidence of associations with weight in the neonatal and infancy periods,18 the anthropometric characteristics and habits of the parents,19 sleep duration,20 exposure to mass media,21 and others.22 Studying these factors is key to the development of efficacious intervention programmes.
In spite of this, most of the research has focused on the adolescent population, with fewer studies devoted to younger children. Furthermore, the high prevalence rates of childhood obesity found in Spain in recent years call for ongoing monitoring to determine the efficacy of the implemented strategies. Thus, the aim of our study was to establish the prevalence rates of childhood overweight and obesity in a representative population of sixth grade students (11 to 12 years of age) in Logroño. We also analysed the sociodemographic factors involved in excess weight, as well as the relationship between excess weight and blood pressure in these schoolchildren.
Materials and methods
Participants
We designed a cross-sectional study of a representative sample of schoolchildren enrolled in the sixth grade of elementary school in the city of Logroño (Spain).The data for that age group during the 2011-2012 academic year corresponded to 1595 students. Assuming an error of 5% and overestimating the number of participants by 20%, schoolchildren were selected by simple random sampling from all the public schools and charter schools (privately-run but subsidised by public funds) in the city, with a participation of 88.4%, resulting in a sample of a total of 329 schoolchildren. The study was conducted during spring of 2012 in each of the schools of Logroño.
Participation of the students was voluntary and in compliance with the ethical principles for medical research of the Helsinki Declaration. We obtained the informed consent of the students' parents or guardians. This study was approved by the clinical research ethics committee of La Rioja.
Sociodemographic data
The study participants reported their own sex, date of birth and country of origin in a questionnaire. The data for their classification into public or charter school students was provided by the Consejería de Educación (Education Dept) of the government of La Rioja. The socioeconomic and sociocultural level of the students was determined based on the information gathered by each of their schools when drawing up their annual educational plan, classified as low, lower-middle, middle, upper-middle, and high. No students fit the high level categories, and the “low” and “lower-middle” categories were combined due to the low number of schoolchildren that fit the former.
Anthropometric measurements
All anthropometric measurements were obtained following the protocol established by the International Society for the Advancement of Kinanthropometry23 and by a single experienced investigator, who had received Level 2 accreditation from that institution.
Weights were measured using a SECA® scale (713, Hamburg, Germany) that was accurate to 0.1 kg. Heights were measured with a Holtain® stadiometer (Holtain Ltd., Dyfed, United Kingdom) accurate to 1 mm. These data were used to calculate the body mass index (BMI) as the weight divided by the squared height (kg/m2). Overweight and obesity were defined according to international criteria.24
Waist and hip circumferences were measured with a Lufkin® flexible steel tape measure (Lufkin W606 PM, Michigan, USA) accurate to 0.1 cm, after which we calculated the waist to hip ratio.
The triceps and subscapular skinfolds were measured with a Holtain® calliper (Holtain Ltd., Crosswell, United Kingdom) accurate to 0.2 mm and with a constant pressure of 10 g/mm2. The percent body fat was estimated using the Slaughter equations.25
Sexual maturation
The level of sexual maturation was determined by trained investigators of the same sex as the participant and by two different methods:
• On one hand, boys self-assessed their maturity stage by reporting the development of their genitalia and pubic hair, while girls self-assessed by reporting the growth of their breasts and pubic hair. Thus, every student assessed their own maturity stage applying the method described by Tanner.26
• On the other hand, we established the age at the “peak growth velocity,” a less subjective method for determining the maturity level by means of equations that use chronological age, sex, and several anthropometric measurements as references.27
Blood pressure
The systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured with a calibrated Riester® (Minimus III, Jungingen, Germany) anaeroid sphygmomanometer and a stethoscope. The measurements were taken with the students in a seated position following more than five minutes of rest and with a cuff appropriate to the size of the child's arm, as indicated by the international consensus recommendations for the evaluation of children.28
The SBP and DBP of each participant were measured in both arms by certified and experienced staff. The measurements were documented in millimetres of mercury (mmHg).
Statistical analysis
Quantitative variables are expressed as mean and standard deviation, and qualitative variables as frequency distributions.
We analysed the association between qualitative variables using Pearson's chi squared test. When the number of cells with expected frequencies of less than 5 exceeded 20%, we used Fisher's exact test or the likelihood ratio test for variables with more than two categories.
We assessed the normality of the distribution by means of the Kolmogorov-Smirnov test or, for smaller samples (n < 30), the Shapiro-Wilk test. Quantitative variables were compared by means of Student's t test or one-factor ANOVA for independent samples, depending on whether two or more groups were being compared. These tests were used for variables with a normal distribution, and the remaining variables were analysed by means of the Mann-Whitney U test and the Kruskal-Wallis test, respectively.
For the one-way ANOVA, we used Welch's robust test of equality of means, and for post-hoc analysis we used the Bonferroni test or the Tamhane test based on whether the variances of the groups being compared were equal or not.
We analysed the data with the statistical software IBM-SPSS® version 20.0 for Windows®. The level of statistical significance was set at 0.05.
Results
The results of our study reflect the anthropometric characteristics of a representative sample of schoolchildren aged 11 to 12 years in Logroño. Table 1 presents the age, sexual maturation, blood pressure and anthropometric characteristics of the participants by sex and by the presence or absence of overweight or obesity. We found no statistically significant differences in any parameter based on the type of school attended other than in age, which was slightly older in public school students (11.8 ± 0.4 years vs 11.7 ± 0.4 years). When it came to country of origin, there were significant differences between Spanish and foreign students-the latter of whom constituted 17.3% of the sample-in the following parameters: age (11.7 ± 0.3 years vs 12.0 ± 0.5 years), Tanner stage (stage 2.3 ± 0.6 vs stage 2.7 ± 0.7), age at peak growth velocity (-2.5 ± 0.4 years vs -2.3 ± 0.5 years) and height (149.3 ± 6.7 cm vs 151.0 ± 8.3 cm).
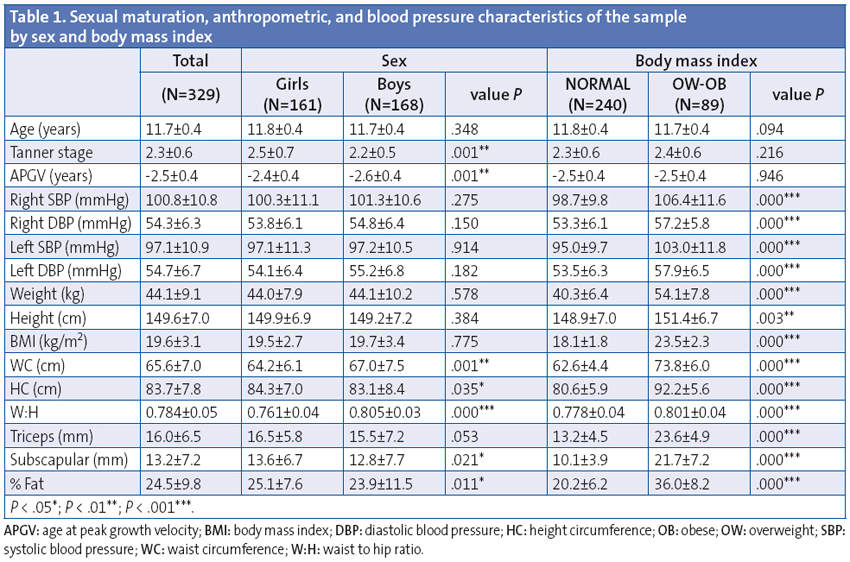
There were significant differences between the sexes in the Tanner scale (stage 2.5 ± 0.7 in girls vs stage 2.2 ± 0.5 in boys), age at peak growth velocity (-2.4 ± 0.4 years vs -2.6 ± 0.4 years), waist circumference (64.2 ± 6.1 cm vs 67.0 ± 7.5 cm), hip circumference (84.3 ± 7.0 cm vs 83.1 ± 8.4 cm), waist to hip ratio (0.8 ± 0.1 vs 0.8 ± 0.0), subscapular skinfold thickness (13.6 ± 6.7 mm vs 12.8 ± 7.7 mm) and percent fat (25.1 ± 7.6% vs 23.9 ± 11.5%), with all values being higher in girls save for the waist circumference. Based on the guidelines of the International Diabetes Federation for children 10 to 16 years of age,29 and using the tables of the nationwide Spanish EnKid study30 as a reference, only 0.6% of the girls and 4.8% of the boys had waist circumference values corresponding to a risk of metabolic syndrome.
When we categorised participants into “normal weight” and “overweight-obese” we found significant differences for all anthropometric and blood pressure variables, with higher values found in the group of children with overweight-obesity in all of them. In this regard, we also found significant correlations (P < .01) between anthropometric variables and blood pressure, both for SBP and DBP and for boys and girls. We found the largest correlations between SBP and weight (r = 0.42 for the right arm and r = 0.43 for the left), waist circumference (r = 0.40 and r = 0.38) and BMI (r = 0.33 and r = 0.5).
The differences in blood pressure for both arms were of 5.4 ± 3.8 mmHg for SBP and 4.0 ± 4.2 mmHg for DBP, with maximum blood pressure values of 15 mmHg reported for SBP in nine schoolchildren and for DBP in eight. Also, hypertension as defined by the International Diabetes Federation29 was found in only two students (< 1%), one of whom was obese and the other overweight.
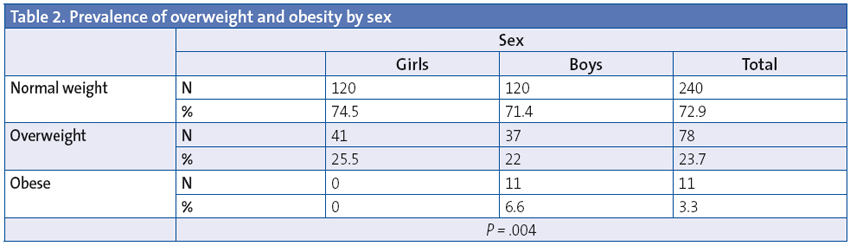
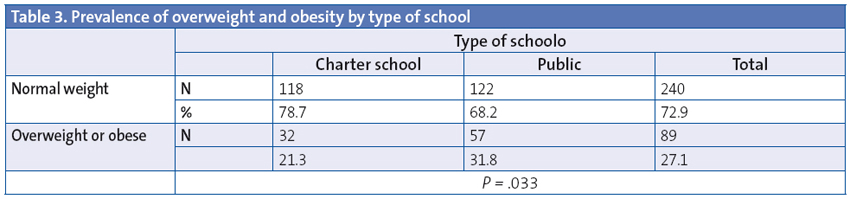
Table 2 shows the distribution of boys and girls in children with normal weight, overweight, and obesity. While the percentages are similar in the normal weight and overweight groups, there were no obese girls, while obesity was found in 6.5% of boys. Continuing with the analysis of the factors that influence excess weight, Table 3 shows that the type of school is one of them too, as the prevalence of overweight and obesity in charter school students was lower than in public school students (odds ratio [OR] = 0.58). We found no significant differences in relation to the country of origin, socioeconomic level or sociocultural level of the students.
Discussion
Our results showed that both sex and the type of school attended are associated with the prevalence of overweight and obesity, with a higher risk of obesity found in boys, and a higher risk of overweight or obesity found in sixth-grade students that attended public schools. In regards to sex, while the prevalence of normal weight was slightly greater in girls, we found a considerable difference between boys and girls in the prevalence of obesity. While a similar trend had been reported in a national study in children 10 to 14 years of age5, with a prevalence of obesity of 4.3% in boys and 3.0% in girls, we ought to note that none of the girls in our sample were obese.
On the other hand, we found significant differences depending on the type of school, with lower percentages of overweight and obesity in charter schools compared to public schools (OR = 0.58). Taking into account the association found between type of school and socioeconomic level (P = .000), this may reflect a considerable difference between public and charter schools in our region, as the same trend has been found in previous studies,31 albeit smaller in magnitude (OR = 0.85). Still, our results did not show any differences in relation to the socioeconomic level of the schoolchildren, although this was not assessed on an individual basis. An important review study17 found a negative correlation between economic level and adiposity in 42% of the reviewed articles, while this correlation was not found in another 27%.
Our study established that 23.7% of schoolchildren are overweight and 3.3% obese. In recent years, studies similar to this one have been performed with non-representative samples of schoolchildren in other Spanish cities, such as Oviedo,32 where obesity percentages of up to 8.4% were reported. Since both populations are located in northern Spain, the differences could be due to the sample not being representative or the larger age interval of participants in the Oviedo study. Still, there are two large national studies on this subject: the EnKid study,33 which found percentages of 22% for overweight and of 5% for obesity in children 10 to 13 years of age; and the latest Encuesta de Salud Nacional (National Health Survey) conducted in Spain,5 which found percentages of 19.2% for overweight and 3.7% for obesity in the 10 to 14 year old population. The percentages of childhood overweight and obesity reported by both studies are similar to those found in our study, which suggests a stabilisation of their prevalence rates in recent years. Nevertheless, these percentages remain very high, as over 25% of schoolchildren aged 11 to 12 years in Logroño were either overweight or obese, a particularly alarming fact considering the negative consequences this has on their present and future health. We must not forget that countries in southern Europe, including Spain, reported childhood obesity prevalence rates that ranged between 6% and 19%, figures that are far removed from the 2% to 4% reported for northern countries.22
In regards to the body fat percentage, Williams34 established the healthy cut-off points at 25% in boys and 30% in girls. In our sample, 35% of boys and 27% of girls exceeded those cut-off points. A study conducted in the United States35 reported body fat percentages of 18.6% for boys and 23.1% for girls in the age group under study. In both cases the figures were below those obtained in our sample. In relation to sex, girls had a higher percent body fat, consistent with previous reports.6
Our analysis of blood pressure found significant relationships between all anthropometric measures (with the exception of the waist to hip ratio) and both systolic and diastolic blood pressure, which had been reported previously in a study of Chinese children and adolescents.2 The latter found that blood pressure increased between 1.4 and 4.1 mmHg with each standard deviation increase in weight, BMI and height. Still, the study most similar to ours considering the age of participants and the geographical location of the sample is the European Youth Heart Study,12 which assessed the blood pressure and anthropometric measures of European children 9 to 10 years of age. This study found the strongest correlations between anthropometric measures and blood pressure in the SBP (r = 0.21 with BMI, r = 0.29 with the waist circumference). While our results showed higher correlation coefficients, which may be due to the older age of our sample, the correlations were also stronger with the SBP in both boys and girls. However, we ought to highlight that only two students had hypertension (less than 1% of the population) and that differences greater than 15 mmHg between both arms in the measurement of blood pressure, which could suggest a risk of vascular disease,36 were not found in any of the participants.
Conclusions
Our results show that the prevalence rates of overweight and of obesity in schoolchildren in the city of Logroño were similar to the national average in the last decade, with the highest prevalence rates found in male students attending public schools. The high prevalence of overweight and obesity underscores the need for intervention programmes that target these high-risk groups.
Funding
This study was partially funded by the Instituto de Estudios Riojanos of the Government of La Rioja per Resolución no. 55, of August 20, 2012 of the Director of the Instituto de Estudios Riojanos for the award of financial grants for scientific studies on subjects concerning La Rioja in 2012.
Conflicts of interest
The authors have no conflicts of interest to declare in relation to the preparation and publication of this paper.
![]() Dirección para correspondencia:
Dirección para correspondencia:
Daniel Arriscado Alsina:
danielarriscado@hotmail.com
References
1. Blair SN. Physical inactivity: The biggest public health problem of the 21st century. Br J Sports Med. 2009;43:1-2. [ Links ]
2. Ma J, Wang Z, Dong B, Song Y, Hu P, Zhang B. Quantifying the relationships of blood pressure with weight, height and body mass index in Chinese children and adolescents. J Paediatr Child Health. 2012;48:413-8. [ Links ]
3. Wang Y, Lobstein T. Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes. 2006;1:11-25. [ Links ]
4. Lobstein T, Frelut M. Prevalence of overweight among children in Europe. Obes Rev. 2003;4:195-200. [ Links ]
5. Encuesta Nacional de Salud 2011-2012. Madrid: Instituto Nacional de Estadística. Ministerio de Sanidad, Servicios Sociales e Igualdad; 2012. [ Links ]
6. Brouwer SI, Stolk RP, Liem ET, Lemmink KA, Corpeleijn E. The role of fitness in the association between fatness and cardiometabolic risk from childhood to adolescence. Pediatr Diabetes. 2013;14:57-65. [ Links ]
7. Freedman DS, Mei Z, Srinivasan SR, Berenson GS, Dietz WH. Cardiovascular risk factors and excess adiposity among overweight children and adolescents: The Bogalusa Heart Study. J Pediatr. 2007;150:12-7. [ Links ]
8. Bell LM, Curran JA, Byrne S, Roby H, Suriano K, Jones TW, et al. High incidence of obesity co-morbidities in young children: A cross-sectional study. J Paediatr Child Health. 2011;47:911-7. [ Links ]
9. Weiss R, Dziura J, Burgert TS, Tamborlane WV, Taksali SE, Yeckel CW, et al. Obesity and the metabolic syndrome in children and adolescents. N Engl J Med. 2004;350:2362-74. [ Links ]
10. Zhou l, Wen SW, He G. Self-esteem situation and relative factor for obese and overweight children. Am J Epidemiol. 2011;173(suppl.11):S125. [ Links ]
11. Brambilla P, Lissau I, Flodmark C, Moreno LA, Widhalm K, Wabitsch M, et al. Metabolic risk-factor clustering estimation in children: To draw a line across pediatric metabolic syndrome. Int J Obes (Lond). 2007;31:591-600. [ Links ]
12. Ruiz JR, Ortega FB, Loit HM, Veidebaum T, Sjöström M. Body fat is associated with blood pressure in school-aged girls with low cardiorespiratory fitness: The European Youth Heart Study. J Hypertens. 2007;25:2027-34. [ Links ]
13. Mitchell JA, Mattocks C, Ness AR, Leary SD, Pate RR, Dowda M, et al. Sedentary behavior and obesity in a large cohort of children. Obesity (Silver Spring). 2009;17:1596-602. [ Links ]
14. Butte NF, Puyau MR, Adolph AL, Vohra FA, Zakeri I. Physical activity in non overweight and overweight Hispanic children and adolescents. Med Sci Sports Exerc. 2007;39:1257-66. [ Links ]
15. Dencker M, Thorsson O, Karlsson MK, Lindén C, Eiberg S, Wollmer P, et al. Daily physical activity related to body fat in children aged 8-11 years. J Pediatr. 2006;149:38-42. [ Links ]
16. Butte NF, Christiansen E, Sorensen TI. Energy imbalance underlying the development of childhood obesity. Obesity (Silver Spring). 2007;15:3056-66. [ Links ]
17. Shrewsbury V, Wardle J. Socioeconomic status and adiposity in childhood: A systematic review of cross-sectional studies 1990-2005. Obesity (Silver Spring). 2008;16:275-84. [ Links ]
18. Olstad DL, McCargar L. Prevention of overweight and obesity in children under the age of 6 years. Appl Physiol Nutr Metab. 2009;34:551-70. [ Links ]
19. Brophy S, Rees A, Knox G, Baker J, Thomas NE. Child fitness and father’s BMI are important factors in childhood obesity: A school based cross-sectional study. PLoS One. 2012;7:e36597. [ Links ]
20. Bell JF, Zimmerman FJ. Shortened nighttime sleep duration in early life and subsequent childhood obesity. Arch Pediatr Adolesc Med. 2010;164:840-5. [ Links ]
21. Council on Communications and Media, Strasburger VC. Children, adolescents, obesity, and the media. Pediatrics. 2011;128:201-8. [ Links ]
22. Ahrens W, Pigeot I, IDEFICS Consortium. Idefics study - Obesity prevalence and risk factors in European children. Am J Epidemiol. 2011;173(suppl.11):S280. [ Links ]
23. Stewart A, Marfell-Jones M, Olds T, de Ridder H. International standards for anthropometric assessment. New Zealand: ISAK, Lower Hutt; 2011. [ Links ]
24. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000;320:1240-3. [ Links ]
25. Slaughter MH, Lohman TG, Boileau RA, Stillman PJ, Van Loan MD, Bembem DA. Skinfolds equations for estimation of body fatness in children and youth. Hum Biol. 1988;60:709-23. [ Links ]
26. Tanner JM, Whitehouse RH. Clinical longitudinal standards for height, weight, height velocity and stages of puberty. Arch Dis Child. 1976;51:170-9. [ Links ]
27. Mirwald RL, Baxter-Jones AD, Bailey DA, Beunen GP. An assessment of maturity from anthropometric measurements. Med Sci Sports Exerc. 2002;34:689-94. [ Links ]
28. National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114(Suppl.2):555-76. [ Links ]
29. Zimmet P, Alberti GK, Kaufman F, Tajima N, Silink M, Arslanian S, et al. The metabolic syndrome in children and adolescents - an IDF consensus report. Pediatr Diabetes. 2007;8:299-306. [ Links ]
30. Serra L, Aranceta J, Ribas L, Sangil M, Pérez C. Crecimiento y desarrollo: dimensión alimentaria y nutricional. En: Serra L, Aranceta J (eds.). Crecimiento y desarrollo. Estudio EnKid, Krece Plus. Vol. 4, Barcelona: Masson; 2003. p. 45-54. [ Links ]
31. Moreno LA, Tomás C, González-Gross M, Bueno G, Pérez-González JM, Bueno M. Micro-environmental and socio-demographic determinants of childhood obesity. Int J Obes Relat Metab Disord. 2004;28 (Suppl.3):S16-20. [ Links ]
32. Martín JJ, Hernández LS, González MG, Méndez CP, Rey Galán C, Guerrero SM. Trends in childhood and adolescent obesity prevalence in Oviedo (Asturias, Spain) 1992-2006. Acta Paediatr. 2008;97:955-8. [ Links ]
33. Aranceta J, Serra L, Foz M, Moreno B, Barbany M, Bellido D, et al. Prevalence of obesity in Spain. Med Clin (Barc). 2005;125:460-6. [ Links ]
34. Williams DP, Going SB, Lohman TG, Harsha DW, Srinivasan SR, Webber LS, et al. Body fatness and risk for elevated blood pressure, total cholesterol, and serum lipoprotein ratios in children and adolescents. Am J Public Health. 1992;82:358-63. [ Links ]
35. Laurson KR, Eisenmann JC, Welk GJ. Body fat percentile curves for US children and adolescents. Am J Prev Med. 2011;41(Suppl.2):S87-92. [ Links ]
36. Clark CE, Taylor RS, Shore AC, Ukoumunne OC, Campbell JL. Association of a difference in systolic blood pressure between arms with vascular disease and mortality: A systematic review and meta-analysis. Lancet. 2012;379:905-14. [ Links ]

