










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Few elderly meet current physical activity (PA) guidelines (Riebe et. al., 2015) of World Health Organization (WHO, 2015) recommendations for maintain or improve cardiorespiratory fitness. The PA can contribute to the harmful changes in which are particularly elevated in postmenopausal women (Choquette et. al., 2011). Although well-established the benefits, the limitations for PA adherence is factors that include aspects anatomical and physiological, level of training, previous experiences (e.g., acquired coping styles or performance strategies), lifestyle factors (e.g., sleep, nutrition), situational cognitive (e.g., self efficacy) and social-psychological (e.g., presence of peers) influences, as well as interactions between these factors (Hall et. al., 2014).
Researches had investigated self-selected exercise effect to provide strategy for health professional to use in PA adherence, and there was observed a greatest tolerance by aerobic exercise practitioners when themselves change intensity during aerobic exercise (Oliveira et. al., 2015) or when they practice PA in outdoor environments (Krinski et. al., 2017). Ekkekakis (2009) suggests self-selected exercise for increase PA adherence, nevertheless it is not clear the evidence about benefits of the method due to no-standardized protocols. When compared to prescribed exercise, the intensity of self-selected exercise shows similar affective answer when compared equal intensity reply in prescribed exercise, but without duration determinate (Oliveira et. al., 2015). On the other hand, there was significate difference in affective answer when the duration was determinated even when the intensity and environment are self-selected (Krinski et. al., 2017).
Despite Krinski et. al., (2017) showed favorable adherence answers when PA is performed with self-selected intensity in environment outdoors the physiological responses obtained, such as percentage maximal oxygen uptake (%VO2max), percentage maximal heart rate (%HRmax), performed during both conditions were similar with intensity of 10% below ventilatory threshold (VT). To optimize benefits in health, there is a necessity of adequate individualized training load, therefore a dose-response relationship should not be under and/or overestimated (Garber et. al., 2011). Therefore, the monitoring training load is an important process to understand self-selected exercise effects.
It is common between coaches and practitioners, during aerobic training program, use heart rate (HR) monitor to for monitoring the training intensity (Braz et. al., 2016) and understand physiological responses, despite not be the single marked to understand the answers. Measure HR, in resting, and HR variables such as HR variability (HRV) can be tools used to inform positive and negative adaptations of aerobic training (Buchheit, 2014). Currently, other tools, for monitoring aerobic training are the subjective parameters scales which have linear relationship with the physiological measures and/or of the external training load, such as rating perceived exertion (RPE) (Kautzner et. al., 2016) and the feeling scale (FS).
The monitoring of training through subjective and objective methods were not discussed in the literature for postmenopausal women. Therefore, the aim of this study was investigate physiological and psychological responses in prescribed and self-selected sessions in postmenopausal women. We believe in the hypothesis of positive affective responses, with low RPE and internal training load (ITL) distinct for self-selected session when compared to the prescribed session.
MATERIALS AND METHODS
The current study was approved by the Research Ethics Committee of the Local Institution, as recommended by Resolution 466/12 of the National Health Council (950.277/2015). Thirty postmenopausal women were selected to participate in the study for convenience in a local physical activity group
Participants
The participants were classified as active according to level of usual physical activity rated by pedometer (9302 ± 3621 steps) (Thompson, Rakow, & Perdue, 2004). All participants signed a consent form, completed a risk stratification (Green, 2010), were healthy and non-smokers. None of the subjects regularly consumed any substance that influenced control tests or currently undergoing hormone replacement therapy.

Experimental Design
A clinical trial was conducted that included 3 sessions at the study sites: (a) initial screening, body composition assessment, incremental shuttle walk test (ISWT) and familiarization session; (b) self-selected session of 20 min; (c) prescribed session of 20 min. Before started each session, the HRV was recorded during 10 min in supine position. Prior of session familiarization were instructed on the methodological procedures and the differences between prescribed and self-selected sessions. In the familiarization session, participants were familiarized with route, besides the scales of RPE, FS and the procedures for self-paced walking. In the self-selected exercise session, participants were allowed to select exercise intensity.
The prescribed session, was performed during the third visit, it was identical o the self-selected exercise session. The physiological variables HR, HRV, % ISWTfinal_stage and psychological variables (Borg 6-20, FS and RPE 0-10) were recorded during and after exercise sessions. The sessions were held in a covered hall well ventilated, with the same temperature and humidity in both sessions. There was a 48 hours interval between the trials. PA levels were classified using the pedometer for the in the 3 days (Stepsaverage_3days).
Psychological Assessments
Whole-body perceived exertion during exercise was obtained using the RPE scale 0-10. Values closer to 0 reflect lower intensity of the session and the closer to 10 reflect higher intensity (Foster, Rodriguez-Marroyo, & De Koning, 2017). The affective valence (pleasure-displeasure) was measured using the FS, which is a single-item 11-point scale ranging from +5 to -5, with verbal anchors of very good (+5), good (+3), fairly good (+1), neutral (0), fairly bad (-1), bad (-3) and very bad (-5). The FS and RPE scale values were measured every 5 min during the experimental sessions, and the presentation of the scales was counter balanced.
The ITL was monitored according to Foster method. The RPE score (s-RPE) was obtained 5 minutes (min) after the end of each session. The subjects individually indicated the degree of perceived exertion according to the Borg CR10 s-RPE. The perceived score reported by the subjects was multiplied by the total session time in min to calculate the ITL (Foster, Rodriguez-Marroyo, & De Koning, 2017). The total ITL corresponds to the sum of the load calculated in the 2 sessions. The data were expressed in arbitrary units (AU).
Physiological Assessments
The analysis of HRV at rest was conducted before training period, in supine position for 10 min without talking or moving. HR data was recorded while spontaneous breathing was monitored and recorded (Buchheit, 2014). HR data were obtained through a Textile Heart Rate Belt (THRB) Firstbeat software version 2.2® (Firstbeat technologies Ltd., Jyväskylä, Finland).
The recorded R-R intervals (iR-R) by THRB Firstbeat software version 2.2® were transferred to a compatible computer. Then, HR signals were processed to calculate HRV using the Kubios HRV® version 3.0.1 (Biomedical Signal Analysis Group, University of Kuopio, Finland). All iR-R with differences greater than 20% of the previous adjacent interval were automatically filtered and inappropriate heart beats were eliminated (low filter).
The iR-R data were analysed in nonlinear methods by variable standard deviations of the Poincaré plot short duration (SD1). Due to the skewed nature of HRV recordings, the SD1 data were transformed into their natural logarithm (Buchheit et. al., 2013; Carlos et. al., 2009).
Incremental Shuttle Walk Test
The Incremental Shuttle Walk Test (ISWT) was obtained in a place marked by cones and length 10m. The initial cadence of .5 m·s-1 was increased by .17 m·s-1 every minute until the subjects showed exhaustion. The speed was controlled by beeps emitted by the Beat Training & Test® (CEFISE, Nova Odessa, Brazil). The test was finished when subject reached exhaustion volunteer. However they were advised to signal any kind of discomfort and that the test could be interrupted at any time or when they did not reach the minimum distance of .5m of the cone at the time of the sound stimulus two consecutives stages (Dourado et. al., 2010). The velocity peak (Vpeak) is represented by the speed in final stage ISWT (ISWTfinal_stage).
Exercise sessions
In the self-selected exercise session, participants determined their intensity exercise. The participants received verbal instruction to perform the exercise in a continuous nature. Thus, the continuous exercise was obtained at a freely chosen pace. Participants were allowed to maintain, increase or decrease the speed in the session.
The time these changes were made, the researchers recorded manually. Participants could stop the exercise session earlier, if they experienced any cardiovascular or pulmonary discomfort and/or musculoskeletal pain. The familiarization session assured a comfortable intensity with the FS and RPE scale during the 20 min.
In self-selected session, the participants maintain a warm up for 3 min at a comfortable speed. Followed an identical protocol familiarization exercise session, 20 min in comfortable intensity, it could be walking or running. The FS answers were obtained every 5 min period (5, 10, 15 and 20min). Any changes in intensity were recorded throughout the 20 min exercise sessions. RPE was recorded at the same moment as the FS.
To prescribed session, the participants maintain a warm up for 3 min at a comfortable speed and then the prescribed exercise intensity was defined. The prescribed session was set same intensity as self-selected exercise session, and the investigator replicated any modifications to the speed that the participants performed in self-selected exercise. This is a similar to approaches used for self-selection in other populations (Hamlyn-Williams, Freeman, & Parfitt, 2014).
Duration and intensity were kept blind from participants so there were not interferences to contribute for FS or RPE (Hamlyn-Williams, Freeman, & Parfitt, 2014), but the participants were told when the speed would changing and whether it would be increased or decreased. The FS answers were obtained in the of each 5 min period (5, 10, 15 and 20min). Any changes in intensity were recorded throughout the 20 min exercise sessions. RPE was recorded at the same moment of the FS.
STATISTICAL ANALYSIS
The normality and homogeneity of the variances were verified using the Shapiro-Wilk and Levene tests, respectively. Prior to analysis, all data were log-transformed for analysis to reduce bias arising from non-uniformity error (heteroscedasticity). The mean, standard deviation (SD) and 95% confidence intervals (CI) were used after the data normality was assumed. A repeated measures analysis of variance (ANOVA) was used to compare HR, SD1, FS, RPE 6-20, time effect (5, 10, 15, and 20 min) x two sessions (Self-selected and Prescribed). ANOVA was followed by Bonferroni post hoc to determine where the significant differences occurred. Assumptions of sphericity were evaluated using Mauchly’s test. Where sphericity was violated (p <.05), the Greenhouse-Geisser correction factor was applied. In addition, effect sizes were evaluated using a partial eta squared (η2p), with < .06, .06-.14 and, >.14 indicating a small, medium, and large effect, respectively. To compare mean values of the descriptive variables, average (20 min) session self-selected vs average (20 min) session prescribed, ITL session self-selected vs ITL session prescribed, a paired t-test was used. The magnitudes of these differences were examined using the standardized difference based on Cohen’s d units by means of effect sizes (d). The d results were qualitatively interpreted using the following thresholds: < .2, trivial; .2-.6, small; .6 - 1.2, moderate; 1.2-2.0, large; and 2.0-4.0, very large.
The relation between variables was determined through the Pearson’s correlation. The confidence interval (95% CI) of the association between variables was calculated. The following criteria were adopted in order to interpret the correlation magnitude: ≤.1, trivial; >.1-.3, small; >.3-.5, moderate; >.5-.7, large; and >.7-.9, very large. If the 95% confidence limits overlapped, small positive and negative values for the magnitude were deemed unclear; otherwise that magnitude was deemed to be the observed magnitude (Hopkins, Marshall, Batterham, & Hanin, 2009). Only clear large (r>.5) correlations were considered. All analyses were conducted in SPSS-22.0 software (IBM Corp., Armonk, NY, USA). The adopted significance was p ≤ .05. The figures were formatted in GraphPad Prism version 6.0 software (La Jolla, CA, USA) following the assumptions for continuous data (Weissgerber, Milic, Winham, & Garovic, 2015). Individualized presentation of the values of the subjects and use of median with interquartile deviation (difference between the 3rd and 1st quartile) for centrality and dispersion measurements, respectively.
RESULTS
Statistical analysis show a significant main effect of the time for HR (F1.121,35.512= 3.771, p= .047, η2p= .115), FS (F1.904,55.207= 5.324, p=.009, η2p= .155) and Borg (F1.353,39.239= 5.958, p=.012, η2p= .170). When observed session by time interaction the significant main effect was noted only in HR (F3,87= 15.340, p<.001, η2p= .346). While time no showed significant main effect for lnSD1 (F1.230,35.675= 2.255, p=.137, η2p= .72) and there was no session by time for Borg (F2,096,60.780= 1.737, p=.183, η2p=.057), FS (F3,87= .626, p= .600, η2p= .021) and lnSD1 (F2.289,66.395= .997, p= .383, η2p= .033).

Table 2 Acute responses to session prescribed and self-selected in women with postmenopausal (n = 30)
Figure 1 show mean and standard deviation values for aerobic self-selected and prescribed sessions feeling scale (1A), Borg 6-20 (1B) and internal training load (1C). A significant difference average was observed for psychological variables FS (M= 3.0, SD= 1.2 vs. M= 3.6, SD= 1.2), t(29)= 2.73, p= .011 (figure 1A), Borg (M= 11,2, SD= 1.7 vs. M= 10.6, SD= 1.9), t(29)= -2.55, p= .016 (figure 1B) and ITL (M= 68 AU, SD= 12 vs. M= 88 AU, SD= 18), t(29)= -5.57, p<.001 (figure 1C). There was no significant different about average values for HR (M= 108 beats/min-1, SD= 11 vs. M= 108 beats/min-1, SD= 11), t (29) = -.277, p= .784, d= .04 (trivial) and lnSD1 (M= 1.8 ms-1, SD= .5 vs. M= 1.9 ms-1, SD= .8), t (29) = 1.211, p= .236, d= -.23 (small). The magnitudes of these differences were small in FS (d= .45) and Borg 6-20 (d= .37), and large for ITL (d= 1.26). Univariate scatterplot (right panels figure 1) shows individual comparison between subjects absolute difference sessions self-selected vs prescribed (raw values). Of the 30 subjects, 22 presented increased in ITL from session prescribed to compared self-selected (mean= 20 AU, 95% CI 13 to 27 AU) and 2 decreased (favor to session self-selected). The results in Borg 6-20 was 18 subjects increased (mean= .7 score, 95% CI .2 to 1.2 score) and 8 decreased. In FS was 18 subjects decreased affective responses (mean= -.5 score, 95% CI -.1 to -.9 score) and 6 increased in favor to self-selected session.

Figure 1 Mean and standard deviation values for aerobic sessions self-selected and prescribed feeling scale (A- black bars), Borg 6-20 (B- white bars) and internal training load (C - gray bars); and individual analysis demonstrated by the univariate scatterplot with median and interquartile deviation of absolute difference (raw value) from aerobic sessions self-selected and prescribed. * = p<.05.
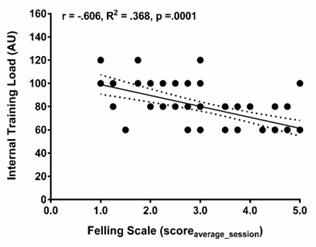
Figure 2 illustrates the correlation between the FS (average session) and ITL. Large negative correlation were observed (r= -.606, R²= .368, 95% CI= -.75 to -.42, p< .001). While no significant large correlation between average session FS and Borg 6-20 were noted.
DISCUSSION
The main findings in the present study were: a) significant difference about the psychological variables (Borg and FS) between prescribed and self-selected sessions, b) physiological responses (HR and lnSD1) to prescribed session were greater in initial 10 min when compared to self-selected, c) more ITL is related to reduction affective responses (22 subjects presented increased in ITL from prescribed session).
The results shown greatest FS and lower RPE answers when self-selected session was performed and significant difference between sessions were observed during the 10 min initial for FS and post 5 min for RPE (table 2). The significant correlation is observed in psychology variables (figure 2). These results are according to Hamlyn-Williams, Freeman, & Parfitt (2014) which shown similar results when intensity in prescribed session was based in self-selected session in female young. It can occur due to the loss in the variable intensity during the exercise session (Ekkekakis, 2009). Aerobic exercise practitioners prefer to change their intensity during aerobic exercise session, despite of no significant difference in affective between self-selected and prescribed sessions (Oliveira et. al., 2015).
Then physiological response, measured trough HR and lnSD1, maintain significant difference during the same period (20 min) as FS answers (table 2). It is due the cognitive processes proposed to dominate in low intensity, however when the increase of this intensity occurs the interoceptive answers tend to be altered (Ekkekakis, 2009). Exercise performed in moderate intensity shows greatest affective answers when compared to high intensity, respectvelly 60-80% VT and 80-90% VT (Ekkekakis et. al., 2008). A mixed between self-selected and prescribed sessions could be included in the training program for PA adherence (Oliveira et. al., 2015). However, the aim in use this strategy to training program has to be adequated to the individual abitlity for maintain or improve health-related parameters. Iellamo et. al., (2014) maintain a key question regarding dose of exercise, and the best mode physical exercise to prescribe to improve of functional ability, due continuous aerobic training and aerobic interval training show similar results and no significant difference. Therefore, the intensity autonomy during aerobic training session for self-selected intensity, could be adequated for analysis prefer practitioners and could increase PA adherence.
Currently it is possible to correlate the %VO2max advocated by Garber et. al., (2011) of 50%-85% for health, with the aerobic activities of hiking and/or race self-selected being represented by a positive affective answer (Smith, Eston, Tempest, Norton, & Parfitt, 2015). Even if the intensity is self-selected, it is presented within the recommended intensity zone for cardiovascular (Dias, Simão, Saavedra, Buzzachera, & Fleck, 2018). Being the use of intensities self-selected in continuous aerobic activity encouraged by health professionals to help ensure program adherence (Ekkekakis, Hall, & Petruzzello, 2008; Hamlyn-Williams, Freeman, & Parfitt, 2014; Smith et al., 2015; McEwan, Arthur, Phillips, Gibson, & Easton, 2018).
In order to bring new evidence in relation to different responses in a self-selected and prescribed session with the same intensity, we identified ITL as something invoker, Iellamo et al. (2013) assessed ITL in individuals with heart failure and found that a moderate dose of exercise, corresponding to approximately 55-60% HR, is sufficient to achieve substantial improvements in HRV. Since affectivity is a subjective parameter that seeks complements RPE (Hardy & Rejeski, 1989) the findings of the present study show a strong relationship between ITL and FS (p< 0,001), with greatest ITL and lower affection in prescribed session and lower ITL and greatest affection in self-selected session, the ITL and RPE relationship corroborate with the previous studies, so the FS encourages future research with new methods.
The results supported by hypothesis, with affective answers being more positive during self-selected session than during the prescribed session, and RPE was lower during the self-selected session than during the prescribed session, beyond greatest ITL for prescribed session despite of being obtained at same intensity.
LIMITATIONS
Among the limitations of the present study we can list the non-use of a direct method for estimation of VO2max as presented in previous studies (Hamlyn-Williams, Freeman, & Parfitt, 2014; Smith et. al., 2015), however, it presents low-cost alternatives to determine physical fitness. The results presented are restricted to the population investigated and may not be applicable in other populations as well as for interval training (Stork, Banfield, Gibala, & Martin Ginis, 2017), in the present study only continuous aerobic training sessions were used, these results may be different for other training methods as well as for other intensities within the continuous method.

