










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.14 no.37 Murcia ene. 2015
ADMINISTRACIÓN - GESTIÓN - CALIDAD
Construct validity and reliability of quality of life instrument family version in Spanish
Validez de constructo y confiabilidad del instrumento calidad de vida versión familiar en español
Barrera Ortiz, Lucy*; Carrillo González, Gloria Mabel*; Chaparro Díaz, Lorena**; Sánchez Herrera, Beatriz*; Vargas Rosero, Elizabeth* and Patricia Carreño, Sonia*
*Master of Nursing. Professor School of Nursing. E-mail: lbarrerao@unal.edu.co
**PhD in Nursing. Professor School of Nursing. National University of Colombia
ABSTRACT
Objective: To determine the construct validity and reliability of the quality of life instrument family version in Spanish, of Betty Ferrell et al.
Method: This is a methodological, descriptive, cross-sectional study. In included the socio demographic characterization of 250 family caregivers of people with chronic illness, from Bogota. The construct validity testing was done with an Exploratory Factor Analysis technique and the reliability with an stability measurement calculating the correlation between the total test and re-test results, and obtaining internal consistency with an alpha of Cronbach's for the global instrument and for each dimension.
Results: The construct validity of the quality of life instrument- family version in Spanish of Betty Ferrell et al, showed the existence of four dimensions: physical, psychological, social and spiritual. The number of factors resulting from the exploratory analysis approached the number of dimensions raised by the authors. The factor analisys of almost 50% of the items correspond exactly to the items designed for measuring each dimension. Discrepancy is observed in the psychological and social dimensions. Regarding reliability tests, the evaluation of the stability found a test-retest correlation of 0.86, and the internal consistency Cronbach's alpha of 0.861 in the test and 0.866 in the re-test.
Conclusions: The quality of life instrument family version in Spanish of Betty Ferrell et al. reported acceptable construct validity and high reliability for its use in the Colombian context. It is recommended to consolidate the construct validity using confirmatory factor analysis techniques to estimate the contribution of an item to one or several dimensions simultaneously and the estimation of possible correlations between dimensions.
Key words: Quality Of Life; Caregivers; Psychometrics; Validity; Reliability.
RESUMEN
Objetivo: Determinar la validez de constructo y confiabilidad del instrumento calidad de vida versión familiar en español de Betty Ferrell y cols.
Método: Estudio metodológico, descriptivo, de corte transversal, que incluyó caracterización sociodemográfica de 250 cuidadores familiares de personas con enfermedad crónica captados en la ciudad de Bogotá; pruebas de validez de constructo por medio de la técnica de Análisis Factorial Exploratorio y de confiabilidad determinando estabilidad, a través del cálculo de la correlación entre los totales del test y el re-test, y consistencia interna obteniendo el coeficiente alfa de Cronbach entre todos los ítems del instrumento y de manera específica para cada dimensión.
Resultados: La validez de constructo del instrumento calidad de vida versión familiar en español de Betty Ferrell y cols. evidencia la existencia de cuatro factores: dimensión física, psicológica, social y espiritual. El número de factores resultante de la solución del análisis factorial exploratorio se aproximó al número de dimensiones planteados por los autores, las cargas factoriales de casi el 50% de los ítems corresponden exactamente con los ítems diseñados y planteados para medir cada dimensión. Se observa discrepancia en las dimensiones psicológica y social. Respecto a las pruebas de confiabilidad, en la evaluación de la estabilidad se encontró una correlación test-retest de 0.86, y en la de la consistencia Interna un alfa de Cronbach de 0.861 en el test y de 0.866 de re-test.
Conclusiones: La escala calidad de vida versión familiar en español de Betty Ferrell y cols. reporta una validez de constructo aceptable y una alta confiabilidad para ser utilizada en el contexto colombiano. Se recomienda consolidar la validez de constructo utilizando técnicas de análisis factorial confirmatorio que permitan estimar el aporte de un ítem a una o varias dimensiones simultáneamente así como la estimación de posibles correlaciones existentes entre las dimensiones.
Palabras clave: calidad de vida; cuidadores; psicometría; validez; confiabilidad.
Introduction
Quality of life (QOL) is a construct conceptualized according to a system of values, standards, or perspectives that vary from person to person, from group to group, and from place to place In consists in the sense of well-being that can be experienced by people and which represents the sum of subjective and personal senses related with "being and feeling well" (2,3).
As a phenomenon of research interest, and tangible indicator of intervention, the concept is quite useful for planning centered on the needs of individuals and the adoption of support models in caring for individuals with chronic disease (4).
Padilla, Grant, and Ferrell (5) indicate that quality of life has a multidimensional connotation characterized by well-being in aspects of life important for the individual. It encompasses the interaction of health and psychological, spiritual, socioeconomic, and family functioning.
Now, in addressing people enduring chronic diseases, it has been recognized that quality of life is a phenomenon that must be explored in the family caregivers, bearing in mind that as agent of care they are affected due to problems produced as a consequence of the long and intense caregiving shifts.
Pinto (6) indicates that it is definite to recognize how the caregiver's life is affected; the caregiver who must live with a person who has a chronic disease. Caregivers are conditioned by different situations that generate overburden, hardship, and dedication, with care being a very demanding task.
It is not easy to confront the fact that a close relative depends on one to continue adapting to their daily life. In most cases, a caregiver assumes that role from one day to the next. This is so because most of the causes of dependence on individuals with chronic disease imply slow and progressive deterioration associated to their increased need for help in their daily life activities.
Assuming the role of caregiver, which is a more or less long process in function of multiple factors, is of dire importance given that it influences substantially on the way care is offered and on the way of feeling. Life changes and it is necessary to make readjustments that permit caregivers to do what they like and as much as they wish.
The quality of life of family caregivers has been assessed through different measurement instruments that have been designed to identify how the caregivers' health and their dimensions are affected upon assuming the care of individuals with chronic disease and who have some degree of dependence (7).
Betty Ferrell et al., (8,9) generated an instrument that measures the quality of life of family members who offer care to a sick relative.
The creation of the scale was based on the theoretical model of quality of life, which was originated in previous studies on quality of life as a measure to assess pain relief, proposed by researchers from the City of Hope Medical Center who define quality of life in terms of four components or dimensions: psychological, physical, social, and spiritual.
The instrument is an adaptation of the QOL patient/cancer survivor instrument, revised and tested between 1994 and 1998 in a study with 219 family caregivers of individuals with cancer. The psychometric tests of the instrument in its original version report a test-retest reliability of r = 0.89, internal coherence with a Cronbach's alpha of r = 0.69. Factor analysis confirmed the four domains of quality of life to be applied in subscales in the instrument. The content validity test was conducted with a group of researchers on quality of life. The second validity test used multiple regression stages; the third was the variance with statistically significant variables for the study with 91% validity and the fourth validity was Pearson's correlation (8).
With respect to the definition of the dimensions: physical well-being refers to control or relief of symptoms and maintenance of function and independence (including functional ability, physical health in general, and symptoms).
Psychological well-being is described as the search for control and in coping with a life-threatening disease and it is characterized by an emotional problem, alteration of priorities, and fear of the unknown, as well as positive changes in life (incorporating the sense of control, depression, fear, and happiness).
Social well-being offers a way of perceiving not only the disease or its symptoms, but also the person within his or her context. It recognizes the subjects with the disease, their relationships, and their roles. It focuses on the negative family stress, social isolation, finance, and sexuality.
Spiritual well-being is the ability to keep hope and obtain meaning from the disease experience, characterized by uncertainty. It contemplates the themes and purpose of life, hope, lack of certainty, and transcendence (9).
Barrera L, Sánchez B, Pinto A, in 2006, with endorsement from the authors, retranslated the instrument into Spanish, adjusted the measurement scale into a Likert-type scale, and adapted it for use with family caregivers of patients with chronic diseases, keeping in mind that conceptual support is closely related with the experiences of the family caregivers of individuals with chronic diseases.
In 2010, Arcos (10) began a validity and reliability process of the instrument Spanish version to be applied in the Colombian context. The author conducted a revision and semantic adjustment of the scale, the face validity, and content validity with experts, reporting a general content validity index (GCVi) of 0.91. For reliability, internal consistency was determined with 108 caregivers measured through Cronbach's alpha of 0.65.
The results of these psychometric tests revealed that only 35 of the 37 items from the original version were pertinent and relevant to assess quality of life in family caregivers of individuals with chronic disease.
Continuing with the psychometric processes to have the Spanish version of the instrument that complies with all the validity and reliability tests required for its use within the local context and addressing the proposal by Arcos, which deleted two items from the original scale, the aim of the present study was to carry out the construct validity and reliability, determining stability through test-retest, and the internal consistency of the scale under question.
Materials and methods
This was a methodological, quantitative, descriptive and cross-sectional study, conducted during the second semester of 2012 as part of a broader Project denominated "Program to diminish the non-transmissible chronic disease burden in Colombia", with 250 family caregivers of individuals with chronic disease in the city of Bogota, who complied with the following inclusion criteria: over 18 years of age, relatives of or close to the sick person, participants in the care decisions, and with over six months involved in the care task.
The subjects were attracted through the solidarity outreach program in the Faculty of Nursing at Universidad Nacional de Colombia "caring for caregivers" and through health institutions caring for individuals with chronic diseases in Bogota.
The instruments used were the caregiver characterization format by the chronic patient care group in the Faculty of Nursing at Universidad Nacional de Colombia and the scale "quality of life family version in Spanish by Betty Ferrell et al.".
Data were taken through direct interview by the researchers and bearing in mind the informed consent in each case. The study considered the ethical aspects regulated by Resolution 8430 of 1993 The environmental policy at Universidad Nacional de Colombia (12) was adhered to, especially on the responsible use of resources. The construct validity was assessed through the Exploratory Factor Analysis technique by using the principal components method and Varimax rotation. The Cronbach-Mesbah Curve (13) was used to verify the dimensionality of the construct of the instrument as a whole and in each dimension.
In validating the construct of an instrument the use of Factor Analysis has been broadly known. Factor Analysis is a multivariate method that seeks to explain a set of observable variables (for this case, the items of the instrument) through a reduced number of non-observable variables called factors (14).
Factor Analysis is a useful technique to investigate the construct validity when the researcher has designed a measure to investigate various dimensions of a phenomenon of interest and wishes to empirically justify these dimensions or factors(13). It is a multivariate method that seeks to explain a set of observable variables (for this case, the items of the instrument) through a reduced number of non-observable variables called factors.
The instrument's reliability was assessed by determining its stability and internal consistency. Assessment of stability was calculated through the correlation between the test and re-test totals; internal consistency through the Cronbach's alpha coefficient among all the items of the instrument and, specifically, for each dimension. To process and analyze the information, the R open code CMC program environment package and the SPSS statistical package version 17.0 were used. Additionally, a professional expert in psychometrics offered statistical advice.
Results and discussion
General characterization of the sample
The family caregivers participating in the study are mostly females (86.4%). With respect to age, most of the caregivers were within the age range over 60 years of age (49.2%), followed by the group from 36 to 59 years of age (27.6%). Regarding schooling, 21.2% of the caregivers had incomplete high school education. The prevailing occupation was homemaker (58%).
Most of the participants stated having more than 37 months in charge of caring for their chronically ill relative (42.8%); the number of hours per day caregivers dedicated to caring for a chronically ill relative is 24 hours per day (55.2%). A total of 60.8% indicate that they are the sole caregiver of the person who is ill.
Caregivers report that the family is the most-frequent (54.4%) support. Lack of support is identified in 24.4% of the participants. Regarding the caregiver-patient relationship, the majority of the caregivers are parents of the person being cared for (43.6%).
Assessment of the construct validity
The construct validity was evaluated through the Exploratory Factor Analysis technique by using the principal components method and Varimax rotation (15). The number of factors resulting from the solution of the Exploratory Factor Analysis was close to the number of dimensions proposed by the author; the factor loadings for 50% of the items correspond to the items designed and proposed by the author to measure each dimension, observing special agreement in the physical and spiritual dimensions. This study used the criteria introduced by Raykov and Marcoulides (16) in 2008 and Waltz et al., (14) 2010, which did not consider significant weighting factors below 0.3 and/or commonality values under 10%.
Table 1 presents the solution for the Exploratory Factor Analysis executed in the test and re-test data, which identifies a solution where four factors are extracted, explaining 42.5 and 44.6% of the variability present in the data, respectively. Each of the four factors extracted explains, in order, 14, 12, 9.5, and 7% of the variability in test data and 13, 13, 9.6, and 9%, respectively, for the re-test data.
The analysis of the effect of the items on the instrument's construct validity permits suggesting that 32 of the 35 items present adequate value of the factor loading of the item over the factor and acceptable commonality value. Item 31 is characterized for having a weighting factor below the accepted limit (<0.3), as well as a commonality value close to the accepted lower limit (0.1); items 11 and 32 present weighting factors and commonality values within the range of accepted values; however, these are found quite close to the permitted lower limit. Values under commonality indicates that much of the variability of the item is not being explained by the factors extracted (Table 1).
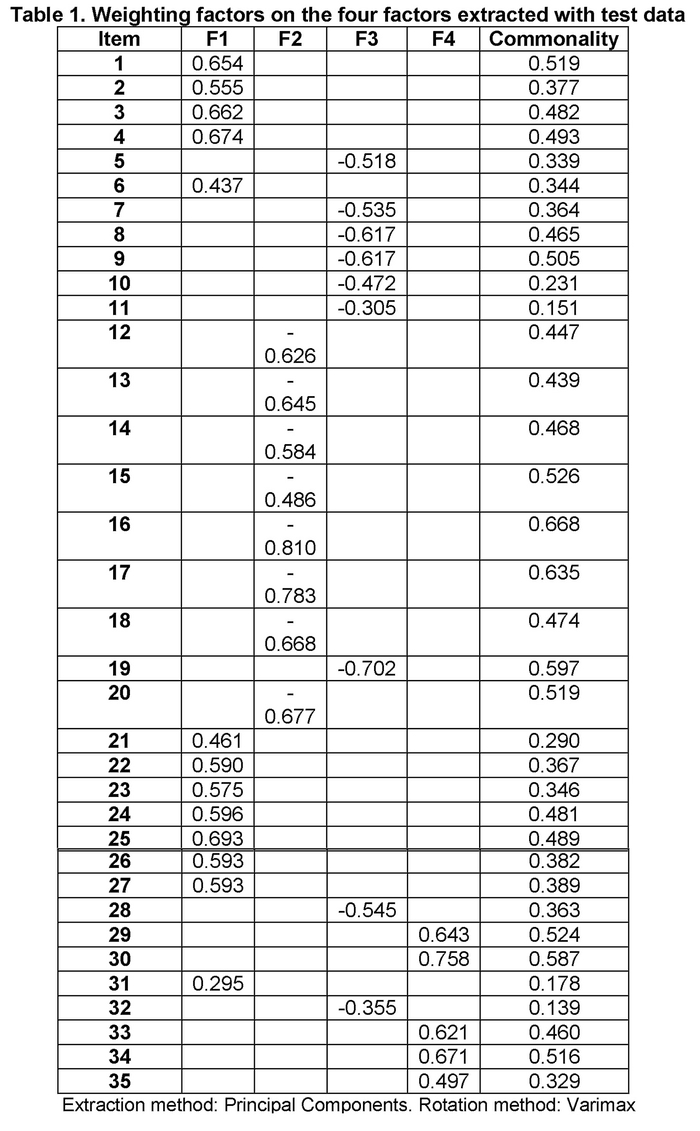
Upon analyzing the factor loading of the items in the four factors extracted and seeking to establish a relationship with the structuring of the dimensions proposed by the authors, 15 of the 35 items are explained by the factor underlying the dimension proposed by the author. An important discrepancy is noted in the Psychological and Social well-being dimensions.
Factor 1 was identified with the Physical well-being dimension. Item 5 is apparently not explained by this factor; however, the solution obtained for the re-test data show a factor loading of 0.555, which is why it was considered an item explained by this factor. The instability observed in the two test and re-test samples suggests that this item's variability may eventually be explained by the effect of Factor 3.
Factor 2 can be identified with a part of the Psychological well-being dimension; items 12-18 are explained between 45 and 67% by this factor. Unlike these, items 7-11 seem best explained by Factor 3. Item 20, in turn, is best explained by this factor, which is not surprising, given that this item assesses the distress experienced, an aspect very akin to Psychological well-being.
Factor 3 can be identified with another part of the Psychological well-being dimension; items 7-10 and 19 are explained to an important proportion by this factor. Item 11 presents a factor loading close to the lowest limit permitted and its percentage of variability explained is close to 10%, identified as an item prone to be removed. Factor 3 was only identified with item 28 of the Social well-being dimension. Items located in this dimension by the author are mostly explained by Factors 2 and 1, thus, Factor 2 (item 20), Factor 1 (items 21-27). Factor 4 is identified with the Spiritual well-being dimension. Items 29, 30, 33, 34, and 35 are explained in percentages above 50% by this factor.
Assessment of reliability
Stability: a test-retest correlation of 0.86 was found. Figure 1 presents the scattergram for the test and re-test data. According to Nunally & Bernstein (13), the satisfactory level for reliability depends on how a measurement is used. In basic research, values for reliability coefficients around 0.8 may be considered adequate.

Assessment of internal consistency of the complete instrument
The Cronbach's alpha coefficient calculated with the test data was 0.861 and with re-test data it was 0.866. These values reflect an adequate degree of internal consistency among the items in the instrument.
Assessment of internal consistency of the instrument per dimension
Upon assessing the internal consistency in each sub-construct, values below 0.8 were found in all the dimensions (Table 2).
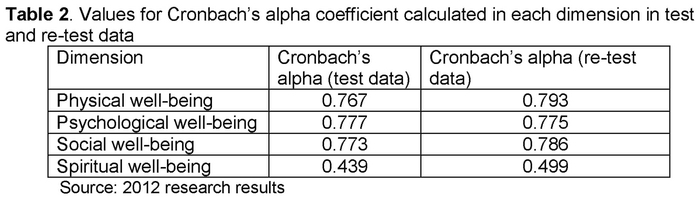
The social well-being dimension identifies that all items contribute favorably to the underlying construct, finding the maximum coefficient value when all the items are present. The Physical well-being dimension shows that item 5 affects the value for the coefficient when eliminating item 5. The Spiritual well-being dimension introduces two items (11 and 12) that affect the construct's reliability. The Spiritual well-being dimension presented the lowest value for the coefficient (0.439 and 0.499 for the test and re-test, respectively). These values are below the desired reliability values in this dimension.
Discussion
The findings from the socio-demographic characterization of this group of caregivers are closely related to those reported in different studies (17,18,19,20).
The quality of life of family caregivers of individuals with chronic disease is constituted as one of the most important key indicators to determine the effect of health interventions upon addressing the burden generated by the care. Hence, having a multidimensional and specific scale on quality of life in family caregivers of individuals with chronic disease, which has all the psychometric requirements to be used within the Colombian context is a factor that will serve as reference point in comprehending and more precise awareness of the situation of family caregivers, becoming a contribution that is required for Colombia to consolidate effective strategies to this situation.
The results obtained in this research are part of the continuity of the psychometric tests from the "quality of life family version in Spanish by Betty Ferrell et al.", reporting for the first time the validity of construct and considered a contribution to the theoretical development proposed by the authors. Part of this contribution is made upon identifying that although the number of factors resulting from the solution of the Exploratory Factor Analysis was able to approach the number of dimensions proposed by the author, the factor loadings of some items do not correspond exactly to those designed and proposed by the authors to measure each dimension.
During the analysis of items, joint assessment of validity and reliability permitted defining elimination criteria in this study without exclusively favoring the instrument's reliability and without risking its construct validity and validity of contents. According to this, items 11, 31, and 32 showed the combination of adverse effect on construct validity and reliability aspects that pose the possibility of their elimination.
We suggest analyzing the construct validity by using confirmatory factor analysis techniques that permit estimating an item's contribution to one or several dimensions simultaneously, as well as estimating possible correlations existing among the dimensions; aspects that cannot be estimated via exploratory factor analysis. Approaching these types of techniques will allow proving hypotheses that lead to validating the construct proposed by the authors.
Additionally, the strength of the scale is identified with respect to reliability by determining the internal consistency and stability, which are considered adequate and are close to those reported by the authors in the original version (8) and surpass that identified by Arcos (10) in 2010.
Carvajal et al., (21) indicate that an instrument's validation is a continuous and dynamic process that acquires greater consistency insofar as more psychometric properties are measured with different populations and subjects.
The findings from the present study support the need to consolidate the scale's validation and reliability process, guaranteeing its quality and accuracy to be used in the local context.
Conclusions
The construct validity of the quality of life family version instrument in Spanish by Betty Ferrell et al., evidences the existence of four factors: physical, psychological, social, and spiritual dimensions. The number of factors resulting from the solution of the Exploratory Factor Analysis came close to the number of dimensions proposed by the author; factor loadings of nearly 50% of the items correspond exactly to the items designed and proposed by the author to measure each dimension. However, discrepancy is noted in the psychological and social dimensions.
The instrument's reliability reports an adequate level. Cronbach's alpha coefficient calculated with the test data was 0.861 and 0.866 with the re-test data. These values reflect an adequate degree of stability and internal consistency among the items of the instrument, with values above those reported the authors of the instrument in its original version.
We recommend consolidating the construct validity by using confirmatory factor analysis techniques that permit estimating the contribution by an item to one or several dimensions simultaneously, as well as the estimate of possible existing correlations among dimensions.
Received: October 29, 2013
Accepted: December 24, 2013
References
1. Velarde Jurado E., Ávila Figueroa C. Evaluación de la calidad de vida. Salud Pública Méx. 2002; 44(4): 349-361. [ Links ]
2. Testa M.A., Simonson D.C. Assessment of quality of life outcomes. N Enl J Med. 1996; 334: 835-840. [ Links ]
3. Gill T., Feinstein A. A critical appraisal of the quality of life measurements. JAMA. 1994; 272: 619-625. [ Links ]
4. Gómez Vela M., Sabeh E. Calidad de vida. Evolución y concepto y su influencia en la investigación y la práctica. Instituto Universitario de Integración en la Comunidad. Facultad de Psicología. Universidad de Salamanca. (Consultado el 15 de julio 2012) Disponible en http://inicio.usal.es/publicaciones.asp. [ Links ]
5. Padilla G., Grant M. y Ferrell B. Nursing research into quality of life. Quality of Life Research. 1992; 1: 341-348. [ Links ]
6. Pinto Afanador N. Calidad de vida del cuidador familiar. En: Grupo de cuidado al paciente crónico y su familia. Cuidando a los cuidadores familiares de personas con enfermedad crónica. Bogotá: Editorial Universidad Nacional de Colombia; 2010. pp.71. [ Links ]
7. Úbeda I. Calidad de vida de los cuidadores familiares: evaluación mediante un cuestionario. (Tesis Doctoral). Barcelona: Universidad de Barcelona. Escuela de Enfermería; 2009. pp. 92-94. [ Links ]
8. Ferrell B. La calidad de las vidas: 1525 voces del cáncer. ONS/Bristol-Myers. Oncology Nursing Forum. 1996; 23(6): 153-159. [ Links ]
9. Ferrell B., Ervin K., Smith S., Marek T., Melancon C. Family Perspectives of ovarian cancer. Cancer practice. 2002; 10(6): 269-276. [ Links ]
10. Arcos D. Validez y confiabilidad del instrumento calidad de vida versión familiar en español. (Tesis Maestría). Bogotá: Universidad Nacional de Colombia. Facultad de Enfermería; 2010. [ Links ]
11. Resolución 8430 de 1993. Por la cual se establecen las normas científicas, técnicas y administrativas para la investigación en salud. Ministerio de Salud de Colombia. Octubre 4 de 1993. [ Links ]
12. Acuerdo 16 de 2011. Por el cual se establece la Política Ambiental de la Universidad Nacional de Colombia. Consejo Superior Universitario. Universidad Nacional De Colombia. 18 de octubre de 2011. [ Links ]
13. Nunally J. and Bernstein I. Teoría Psicométrica. 3ra. Ed. México: Mc-Graw Hill; 1995. pp. 296-297. [ Links ]
14. Waltz C., Strikland O., and Lenz E. Measurement in Nursing and Health Research. 4th Ed. New York: Springer Publishing Company; 2010. [ Links ]
15. Lucero I., y Meza S. Validación de instrumentos para medir conocimientos. Argentina: Departamento de Física. Facultad de Ciencias Exactas y Naturales y Agrimensura - UNNE; 2002. (en línea) (citado el 4 de Diciembre 2010) Disponible en: http://www1.unne.edu.ar/cyt/2002/09-Educacion/D-027.pdf. [ Links ]
16. Raykov T., and Marcoulides G. An Introduction to Applied Multivariate Analysis. New York: Routledge; 2008. pp. 265. [ Links ]
17. Vanegas B.B. Habilidad del cuidador y funcionalidad de la persona cuidada. Aquichan. 2006; 1(6):137-147. [ Links ]
18. Barrera L., Pinto N., Sánchez B., Rocio C., Moreno M., Pinzón L., et al. La habilidad de cuidado de los cuidadores familiares de personas con enfermedad crónica: Un estudio comparativo en tres unidades académicas de enfermería. Investigación y Educación en Enfermería. 2006; 24(1): 36-46. [ Links ]
19. Montalvo A., Flórez I. Características de los cuidadores de personas en situación de cronicidad. Cartagena Colombia. Un estudio comparativo. Salud Uninorte. 2008; 24(2): 181-190. [ Links ]
20. Moreno Moreno J.A., Arango Lasprilla J.C., Rogers H. Necesidades familiares y su relación con las características psicosociales que presentan los cuidadores de personas con demencia. Psicología desde el Caribe (revista en línea). 2010; (26): 135. (consultada el 07 de julio de 2013). Disponible en: http://rcientificas.uninorte.edu.co/index.php/psicologia/issue/view/35. [ Links ]
21. Carvajal A., Centeno C., Watson R., Martínez M., Sanz A. ¿Cómo validar un instrumento de medida de la salud? An. Sist. Sanit. Navar. 2011; 34(1): 63-72. [ Links ]

