










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkEnfermería Global
On-line version ISSN 1695-6141
Enferm. glob. vol.15 n.41 Murcia Jan. 2016
CLÍNICA
Therapeutic management of users with oral anticoagulant therapy
Gestão terapêutica dos utentes com terapia anticoagulante oral
Manejo terapéutico de los usuarios con terapia anticoagulante oral
Serra, Isaura da Conceição Cascalho*; Ribeiro, Lurdes da Conceição Afonso Nobre**; Gemito, Maria Laurência Grou Parreirinha*** and Mendes, Felismina Rosa Parreira****
*UCP, Doctoral student in Nursing; Master's Degree in Socio-Organisational Intervention in Health; Assistant Professor at the University of Évora - S. João de Deus School of Nursing. E-mail: iserra@uevora.pt
**Master's Degree in Community Nursing; Degree in Nursing from Ponte de Sôr Medical Centre
***PhD in Sociology, Assistant Professor at the University of Évora - S. João de Deus School of Nursing, Researcher at the Health Sciences and Technology Research Centre of the University of Évora.
****PhD in Sociology. Coordinating Professor of the S. João de Deus School of Nursing of the University of Évora. Researcher at the Centre for Research and Studies in Sociology of the Lisbon University Institute (CIES/ISCTE-IUL) Portugal.
ABSTRACT
Objective: Characterize the users of oral anticoagulant therapy; to find out about treatment regimen management and to estimate International Normalized Ratio (INR) assessment costs.
Methodology: Descriptive, exploratory, cross-sectional study with 83 users of oral anticoagulant therapy from a primary health care centre in Alentejo (Portugal). Data collection occurred with the application of a questionnaire designed for the purpose.
Results: It was found that 50.6% reported that they did not know what clotting is; 49.4%, what oral anticoagulants are; 63.9%, what the complications are of oral anticoagulant therapy. Only 27.7% know the foods that interfere with this therapy, and 51.8% mentioned that they knew what to do in the event of injury, tooth extraction or surgery. INR assessment costs in the laboratory are higher than in the primary health care centre.
Conclusions: Gaps in knowledge regarding coagulation, food interference and treatment regimen were identified. The decentralisation of nursing appointments enables costs to be reduced, improves accessibility and management of the treatment regimen.
Key words: Community Health Nursing; Patient Care; Disease Management; Therapeutics; Anticoagulants.
RESUMO
Objetivo: Caraterizar os utentes com terapia anticoagulante oral; conhecer a gestão do regime terapêutico e estimar custos da avaliação de Razão Normatizada Internacional (RNI).
Metodologia: Estudo descritivo, exploratório, transversal, realizado com 83 utentes com terapia anticoagulante oral de um Centro de Saúde do Alentejo (Portugal). A coleta dos dados ocorreu com aplicação de questionário construído para o efeito.
Resultados: Concluiu-se que 50,6% referiram não saber o que é coagulação; 49,4% o que são anticoagulantes orais; 63,9% quais as complicações da terapêutica anticoagulante oral. Apenas 27,7% conhecem os alimentos que interferem com esta terapêutica e 51,8% mencionam saber o que fazer em caso de ferida, extração de dente ou cirurgia. O custo da avaliação de RNI em laboratório é mais elevado que nos Centros de Saúde.
Conclusões: Identificaram-se lacunas nos conhecimentos sobre coagulação, interferências alimentares e regime terapêutico. A descentralização da Consulta de Enfermagem permite reduzir custos, melhorar a acessibilidade e gestão do regime terapêutico.
Palavras chave: Enfermagem em Saúde Comunitária; Atenção ao paciente; Gerenciamento Clínico; Terapêutica; Anticoagulantes.
RESUMEN
Objetivo: Caracterizar a los usuarios con terapia anticoagulante oral; conocer el régimen de tratamiento y estimar los costes de evaluación de la International Normalized Ratio (INR).
Metodología: Estudio descriptivo, transversal, exploratorio, con 83 usuarios con terapia anticoagulante oral de un Centro de Salud de Alentejo. Los datos fueron recolectados con la aplicación de cuestionario construido para este fin.
Resultados: Se concluyó que 50,6% informaron no saber qué es la coagulación; 49,4% lo que son anticoagulantes orales; 63,9% las complicaciones de la terapia anticoagulante oral. 27,7% conoce los alimentos que interfieren con esta terapia y 51,8% declara saber qué hacer en caso de lesión, cirugía o de la extracción de un diente. El costo de la evaluación de RNI (Razón Normalizada Internacional) en laboratorio es mayor que en los centros de salud.
Conclusiones: Existen lagunas en el conocimiento sobre el proceso de coagulación, la interferencia de alimentación y el régimen. La descentralización de la consulta de enfermería puede reducir los costos, mejorar la accesibilidad y la gestión del régimen terapéutico.
Palabras clave: Enfermería en Salud Comunitaria; Atención al Paciente; Manejo de la Enfermedad; Terapéutica; Anticoagulantes.
Introduction
Cardiovascular diseases are a group of diseases that affect the cardiovascular system, specifically the heart and blood vessels. Their consequences are often sudden and unexpected, sometimes culminating in the death of the person. The control of risk factors and effective management of the therapy regimen may contribute to a reduction in fatal and non-fatal complications of cardiovascular diseases(1)
With an ageing population and its impact in terms of health and current eating habits, the situation is likely to worsen. According to the United Nations (UN), the world's elderly population is growing 2% each year and the proportion of elderly is growing faster than any other age group. Around the year 2050, the elderly will represent one 1/5 of the elderly(2). Investments must be made in education in order to prevent these diseases and their consequences.
"The high domestic prevalence of risk factors for cardiovascular diseases requires particular attention to be paid to effective prevention, detection and correction, taking into account that the concept behind this term incorporates not only action that prevents a loss of health, but also all care that promotes recovery. It also requires the adoption of integrated and complementary measures that foster, among the Portuguese population, a reduction in the risks of contracting these diseases, prompt and appropriate treatment and secondary prevention measures that reduce their recurrence"(3)
Some examples of situations where oral anticoagulant therapy (OAT) is recommended are: the prevention of deep vein thrombosis and pulmonary embolisms; the prevention of clots and emboli in patients with artificial heart valves; preventing the formation of clots and emboli in patients with atrial fibrillation and prevention of myocardial infarction in some patients with specific characteristics. It may also be considered for patients who are to undergo complicated surgery or those that require prolonged immobilisation(4).
Oral anticoagulants are used within the framework of primary and secondary prevention of thromboembolic events, so there are a large number of patients using this type of medication prescribed for long periods of time. Effective management of the treatment regimen is important as, where a disease situation is concerned, there is often a need to change lifestyles, which is not always accepted by patients, resulting in risks to health and the prevention of complications; at the same time, determining the appropriate therapeutic dose of these drugs is also complex.
According to the Ministry of Health, around 40% of deaths recorded in Portugal are due to cardiovascular disease, and half of these deaths are the result of cerebral vascular problems. Pathological conditions such as atrial fibrillation (AF) lead to a high number of patients having to undergo daily anticoagulant therapy to prevent thromboembolic events such as stroke. It is estimated that there are approximately 100 thousand patients taking anticoagulants in Portugal, this number increasing significantly every year(1).
The haemostatic system comprises an entire vascular endothelium and platelets and coagulation factors in the bloodstream. Its main function is to maintain the fluidity of the blood and stop bleeding when a vascular injury occurs. Complete balance is required between the coagulation, or fibrin formation, mechanisms and the fibrinolytic, or fibrin destruction, mechanisms. Oral anticoagulants derived from 4-hydroxycoumarin (acenocoumarol and warfarin sodium) are indirect action anticoagulants that reduce the hepatic synthesis of factors II, VII, IX and X of the coagulation, by antagonising the action of vitamin k (phytomenadione). Unlike heparin, they have no anticoagulant effect in vitro. The most representative drug is warfarin; acenocoumarol is used less frequently. They prolong prothrombin time (PT), which assesses the integrity of the extrinsic system and is used to control the anticoagulant effect; it is referred to as the INR (International Normalised Ratio); they also increase the activated partial thromboplastin time (APTT), which measures the integrity the intrinsic system. Coumarin-type oral anticoagulants (e.g., warfarin and acenocoumarol) act by blocking, at the hepatocyte level, the carboxylation of vitamin K-dependent proteins, and are increasingly used in primary and secondary prophylaxis of thromboembolic disease(4). Despite better definition of the therapeutic areas and greater standardisation of laboratory monitoring, these drugs are not free from haemorrhagic and thromboembolic complications, often consequences of an excessive anticoagulant effect and insufficient anticoagulation, respectively. Thus, it becomes essential to monitor them by means of laboratory tests to ascertain prothrombin time (expressed in INR)(5.7)
The literature reveals that the majority of OAT patients are female, with an average age close to 60 years of age, married, retired, with associated diseases, which have been undergoing this therapy for more than 5 years, with INR valueswithin the therapeutic parameters(6-7). The use of OAT requires care in order to maintain levels of blood coagulation under control and prevent thromboembolic or haemorrhagic complications. Sometimes such care can lead to changes in lifestyle, changes in dietary habits, alcohol consumption, daily intake of medication, observation consultations and fear of complications, which may compromise the quality of life of these people(7).
Users of oral anticoagulant therapy need to be monitored once or twice a month to control the therapeutic dose, taking into account the levels of anticoagulation and the dangers of overdose. According to the figures agreed by the guidelines of the seventh conference of the American College of Chest Physicians, the target INR value should be equal to 2.5 ± 0.5 and a nursing consultation at the primary health care centre has the advantage for the patient of offering more frequent tests, with less risk of bleeding and its effects, increased independence and with results as reliable as the laboratory method, with dosing being changed immediately after determination of the INR(8) Accordingly, the existing human and physical resources should be managed and focused on allowing access to the widest number of users who are dependent on them, in order to reduce the mortality and morbidity of these diseases(9). The policy of decentralisation aims to delegate roles and/or decision-making, charging other professionals with performing the same tasks at another location. Decentralising the Anticoagulation Consultation and the monitoring of INR in hospitals or clinical analysis laboratories to primary health care centres enables patients to get closer to the health care they need, ensuring greater accessibility and proximity, at a lower cost.
This study aims to: Identify and characterise users of oral anticoagulant therapy; analyse treatment regimen management and estimate INR (International Normalized Ratio) assessment costs.
Methodology
A descriptive, exploratory, cross-sectional study taking a quantitative approach. The study population consists of the total number of users of oral anticoagulant therapy registered at a primary health care centre in Alentejo (Portugal), a total of 83, whose selection criteria consisted of being over 18 years of age and undergoing monitoring of INR and respective control of the therapeutic dose at that primary health care centre, after informed consent. For data collection, a questionnaire was applied, which had been previously tested on a sample population with characteristics similar to those of the study population. The questionnaire was developed based on the literature consulted in order to meet the objectives and, despite the various possible components of the management of the treatment regimen, only the cognitive component was considered.
The first part intends to provide a socio-demographic description of the users, and the second asks some questions in order to evaluate the patients' perception and knowledge regarding coagulation, what oral anticoagulants are, the complications of this type of therapy, the information they have about the correct way to take the medicine, what to do in the event of forgetting a dose, the importance of attending for INR assessment on the established dates, considering whether the anticoagulant patient can/should live a normal life, which medicines may be taken, foods that interfere with oral anticoagulant therapy and care in the event of injury, the need to extract a tooth or undergo surgery.
The questionnaire was given to the patients when they attended the primary health care centre for INR monitoring and control of the respective therapeutic dose.
In order to meet the latter objective, i.e. to estimate the costs of INR assessment, the respective calculations were prepared for evaluation in a clinical laboratory at the primary health care centre and main advisory services. The cost of the INR analysis tabulated by Ordinance no. 839-A/2009 of 31 July was used as a reference.
In assessing the costs, essentially user-centred parameters were considered, except for the cost of the analysis, which did not take into account the costs involved in technicians' work.
All ethical procedures were followed (informed consent, confidentiality and anonymity) in accordance with the Declaration of Helsinki on Ethics in Research Involving Humans.
Descriptive statistical processing of the data then followed, using relative and absolute frequencies, by means of the Statistical Package for the Social Sciences (SPSS®)18.0.
Results
After analysing the data, we could conclude that most of the users of oral anticoagulant therapy that responded are female (56.6%) and 71 to 80 is the age group with the largest number of patients (43.4%), most are married (67.5%), immediately followed by widows (24.1%). Most have already retired (86%). With regard to knowledge about what coagulation is, 50.6% stated that they have no knowledge regarding this subject. However, despite the previous response when several hypotheses have been submitted to choose, 50.6% of respondents recognized that coagulation is a natural process that enables the body to reduce blood loss in case of bleeding. In relation to users' knowledge regarding what oral anticoagulants are, around 50.6% answered affirmatively, considering them to be medicines that cause the blood to take longer to coagulate. It may also be concluded that most users of oral anticoagulant therapy (63.9%) do not know the complications associated with OAT. Patients who claim to know what the complications of oral anticoagulant therapy are mentioned the main complication as being bleeding. The data show that 63.9% know what to do if they forget a dose of the oral anticoagulant, but around a quarter of this group does not adopt the correct procedure if they forget one. It was also observed that 60.2% know what drugs may be taken while undergoing OAT. The results indicate that the majority of users surveyed (72.3%) reported not knowing which foods interfere with OAT. In relation to precautions to be taken in the event of injury, the need for tooth extraction or surgery, 51.8% responded correctly.
It resulted from the analysis of the data that 94% of those surveyed believe that an user of oral anticoagulant therapy can and should live a normal life, reinforcing the importance of attending INR evaluations on the established dates, and the 6% who made reference to the limitations that compromise their normal life accentuate increased care in relation to the risk of falls, wounds and cuts that may trigger bleeding.
The majority of patients (85.5%) report having information that they should only undergo the therapy prescribed by the doctor, and only after informing that, they are undergoing OAT.
Another objective of the study was to estimate the costs of INR assessments. The importance of this objective lies in the fact that this patients need to monitor their INR values once or twice a month in order to control the prescribed therapeutic dose, bearing in mind the levels of anticoagulation and the risk of overdose. Accordingly, a plan was drafted for their evaluation in a clinical laboratory at the health care centre and main advisory services, thus avoiding patient visits, which ended up reducing costs considerably. Taking the INR cost analysis tabulated by Ordinance no. 839-A/2009 of 31 July(10) as a reference (4.70 €), a simulation was carried out of the costs at the various sites where it is possible for the study population to evaluate INR, as per Table I.
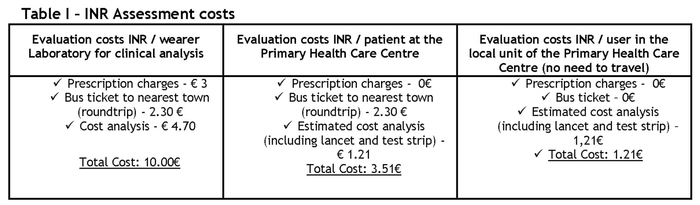
We can thus conclude that INR assessment in a clinical laboratory is, undoubtedly, the most expensive, followed by evaluation at the health care centre, taking into account that the patient will have to travel from one parish to the county town, it thus being more economical to decentralise the nursing consultation and the INR assessment for patients undergoing oral anticoagulant therapy to the health advisory services. The decentralisation of nursing appointments for those patients thus enables costs to be reduced, improves accessibility and promotes more effective management of the treatment regimen.
Discussion
Most patients know that coagulation is a natural process that enables the body to reduce blood loss in the event of bleeding and that OAT makes the blood take longer to coagulate. Most say that they do not know the complications of OAT, but report the bleeding as the main complication. Studies indicate that bleeding is the most common adverse event(11,12). Fear of bleeding may sometimes lead to high anxiety levels, especially in people who have already been through this situation(7).
They also mention being informed by their doctor about the proper way to take the OAT and how to proceed in the event of forgetting a dose. Almost all of the respondents consider it important to meet the INR assessment dates, and see no reason not to carry on a normal life, whereby, when there is reference to the reasons that prevent a normal day-to-day life, they point to increased precautions in relation to the risk of falls and cuts that may trigger bleeding. Studies indicate that the quality of life assessment showed the worst among elderly women who have been undergoing the therapy for less than one year. The highest quality of life is related to social aspects and the worst inherent to the physical aspects(7).
With respect to the foods that interfere with OAT, many doubts and a lack of knowledge were identified. The dose of anticoagulant should be adjusted in accordance with a healthy diet, and never the opposite. The way in which the INR value responds to the consumption of various types of vegetables also varies from individual to individual, and so it is critical to maintain regular control of the INR(11,13,17). It may also be concluded that, in relation to the precautions to be taken in the event of injury, the need to extract a tooth or undergo surgery, the patients state that they know what attitudes to adopt, except in the case of the need to extract a tooth. These recommendations are crucial and health professionals must be made aware of these issues(11). However, one study indicates that although the majority of doctors (60%) questioned patients about using OAT during consultations, they demonstrate insufficient knowledge about this subject, and 92% are interested in knowing more about OAT(12).
The study also enabled us to conclude that INR assessment in a clinical laboratory is, undoubtedly, the most expensive (10.00€), followed by evaluation at the health care Centre, taking into account that the patient will have to travel from one parish to the county town (3.51€), it thus being more economical to decentralise the Nursing Consultation for patients undergoing OAT to the health advisory services (1.21€). A cost-effectiveness and cost-utility study carried out in Portugal has enabled a comparative analysis to be undertaken of costs, years of life and quality of life, considering that INR valuescould be self-monitored, monitoring at a primary health care centre and monitored at a clinical laboratory. It was found that self-monitoring is an alternative that is more beneficial in terms of gain in years and quality of life and alternative monitoring in a clinical laboratory is one that offers less benefits, both in terms of gains in years of life and quality of life. In relation to direct costs, monitoring at primary health care centres offers the lowest costs, as opposed to monitoring in a laboratory, which involves the highest costs. The researchers concluded that both self-monitoring and monitoring at a primary health care centre are dominant in relation to monitoring at a clinical laboratory, both involving lower direct and indirect costs and greater gains in terms of years of life and quality of life(8).
This decentralisation facilitates access to, not only quality, but also timely health care, taking a holistic view of the patient at the most appropriate location for the target population. The National Health Plan 2012-2016 states that the "adequate access is one of the determinants of health, as it enhances the reduction of inequalities"(15).
Conclusions
Health is a fundamental human right and an indispensable factor for the economic and social development of any region. Health Promotion is an essential process of empowering patients to control and improve their health. Acting on the determinants of health not only contributes to health gains, but also reduces inequalities and hence the promotion of fundamental rights of the human being. Health should be understood as a resource for life, i.e. the user must be proactive, learning skills to take maximum responsibility and autonomy, modifying behaviours and thereby promoting self-care.
We may conclude by analysing the data that there are some gaps in relation to knowledge that user of oral anticoagulant therapy possess in relation to the management of the treatment regimen, including knowledge of the coagulation process, food and drug interference and execution of the OAT. The guidelines of the National Health Plan 2011-2016 defend a health system whose conceptual model seeks to maximise health gains through sustained effort from all sectors, with emphasis on equity and access to quality health policies geared towards reducing inequalities.
Thus, it is suggested that, in order to empower these patients, education sessions on health, both individual and in groups, on food, drug interactions and management of the therapeutic regimen should be scheduled. Decisions related to health cease to be almost exclusively centred on professionals and move towards the patient who is the subject of the care. This paradigm shift demonstrates that reflection on the value of personal autonomy has led health professionals to rethink the role of patients, leading to them being gradually integrated into decision-making and health care planning(14).
In fact, "the changes in the demographic profile, the indicators of morbidity and the emergence of chronic diseases translate into new health needs, the role of primary health care having been recognised in recent years, with emphasis on responsiveness in solving the problems posed by citizens in order to form a strong and dynamic society"(16).
It seems interesting to us to, in the future, established interventions for this population, in order to bridge the gaps found in terms of knowledge and evaluate their health-related quality of life, for which a tool such as the Medical Outcomes Survey 36 - Item Short-Form (Sf-36), in the validated Portuguese version, may be used(7).
Received: September 23, 2014
Accepted: November 1, 2014
References
1. Ministério da Saúde (PT). Doenças Cardiovasculares (internet). (publicado em 2009 out 1; acesso em 2011 jul 22). Disponível em: http://www.min-saude.pt/portal/conteudos/enciclopedia+da+saude/doencas/doencas+do+aparelho+circulatorio/doencascardiovasculares.htm. [ Links ]
2. Assis M. Promoção da Saúde e Envelhecimento: avaliação de uma experiência no ambulatório do Núcleo de Atenção ao Idoso da UnATI/UERJ (tese). Rio de Janeiro: FIOCRUZ/Escola Nacional de Saúde Pública; 2004. [ Links ]
3. Ministério da Saúde (PT), Direção-Geral da Saúde. Despacho no 16415/2003 (II série). D.R. no. 193 de 22 de Agosto: Programa Nacional de Prevenção e Controlo das Doenças Cardiovasculares. Lisboa; 2003. [ Links ]
4. Infarmed. Anticoagulantes Orais (internet). (acesso em 2011 abr. 20). Disponível em: http://www.infarmed.pt/prontuario/navegavalores.php?id=119. [ Links ]
5. Barreira R, Ribeiro J, Farinha M, Martins R, Rodrigues I, Mendes Z, et al. Monitorização da Terapêutica com Anticoagulantes Orais: Consulta de Anticoagulação vs Médico Assistente. Acta Med Port. 2004; 17: 413-6. [ Links ]
6. Pelegrino FM, Dantas RAS, Corbi ISA, Carvalho ARS. Perfil sócio demográfico e clínico de pacientes em uso de anticoagulantes orais. Rev. Gaúcha Enferm. 2010; 31(1): 123-8. [ Links ]
7. Corbi ISA, Dantas RAS, Pelegrino FM, Carvalho ARS. Qualidade de vida relacionada à saúde de pacientes em uso de anticoagulação oral. Rev. Latino-Am. Enfermagem. 2011; 19(4): 865-873. [ Links ]
8. Macedo A, Carrasco J, Andrade S, Moital I. Estudo de Avaliação do Custo Incremental da Auto-Monitorização de INR versus Controlo Laboratorial ou Monitorização no Centro de Saúde, em Portugal. Acta Med Port. 2010; 23: 203-212. [ Links ]
9. Ministério da Saúde (PT), ARS do Centro. Plano de Ação 2010. Coimbra (internet). (publicado em 2010 março; acesso em 2011 maio 22). Disponível em: http://pns.dgs.pt/files/2010/02/Plano-de-Acção-2010-Administração-Regional-de-Saúde-do-Centro.pdf. [ Links ]
10. Ministério da Saúde (PT). Portaria no839-A/2009 de 31 de Julho: Tabelas de preços a praticar pelo Serviço Nacional de Saúde, bem como o respetivo Regulamento. Diário da República, Lisboa 2009 jul 31; 147 1.a série: 4978-(2). [ Links ]
11. Quintero-González JA. Cincuenta años de uso clínico de la warfarina. Investigación Clínica. 2010; 51(2): 269-287. [ Links ]
12. Borlina LP, Silva ELC, Ghislandi C, Timi JRR. Conhecimento sobre anticoagulantes orais e seu manejo por médicos de pronto atendimento. J Vasc Bras. 2010; 9 (2): 24-8. [ Links ]
13. Associação Portuguesa de Doentes Anticoagulados. Dieta & Interações (internet). (acesso em 2011 fev. 2). Disponível em: http://www.apda.com.pt. [ Links ]
14. Dias MR, Duque AF, Sila MG, Durá E. Promoção da Saúde: O renascimento de uma ideologia?. Análise Psicológica. 2004; 3 (XXII): 463-473. [ Links ]
15. Ministério da Saúde (PT). Plano Nacional de Saúde 2012-2016 (internet). (publicado em 2011 fev. 4; acesso em 2011 abr. 10). Disponível em: http://www.acs.min-saude.pt/pns2011-2016/files/2011/02. [ Links ]
16. Ministério da Saúde (PT). Regulamento no 128/2011 de 18 fevereiro de 2011: Regulamento das Competências Específicas do Enfermeiro Especialista em Enfermagem Comunitária e de Saúde Pública. Diário da República, Lisboa 2011 fevereiro 18; 35 2.a série: 8667-8669. [ Links ]
17. Esmerio FG, Souza EN, Leiria TL, Lunelli R, Moraes MA. Uso crônico de anticoagulante oral: implicações para o controle de níveis adequados. Arq. Bras. Cardiol. 2009; 93(5): 549-554. [ Links ]

